You might also like
- Adverse Blood Reaction and HDNDocument34 pagesAdverse Blood Reaction and HDNAdeniran CharlesNo ratings yet
- Complications of Blood TransfusionDocument18 pagesComplications of Blood TransfusionIqra ghafoorNo ratings yet
- Transfusion Reaction - DRGSPDocument42 pagesTransfusion Reaction - DRGSPGaurav PawarNo ratings yet
- HPB Adverse Transfusion ReactionDocument26 pagesHPB Adverse Transfusion ReactionFransiscus RivaldyNo ratings yet
- Serious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologyDocument65 pagesSerious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologySuneil R AlsNo ratings yet
- Blood ProductsDocument70 pagesBlood Productsjadhamade339No ratings yet
- Transfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1Document33 pagesTransfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1UmikaguptaNo ratings yet
- Blood Transfusion and Its ComplicationsDocument31 pagesBlood Transfusion and Its ComplicationsSaima Hasnain MinhasNo ratings yet
- Approach and Management of Bleeding NeonateDocument49 pagesApproach and Management of Bleeding NeonateG VenkateshNo ratings yet
- Adverse Reactions To Blood Transfusion1Document38 pagesAdverse Reactions To Blood Transfusion1Abby Liew100% (1)
- 5 Transfusion ReactionsDocument20 pages5 Transfusion ReactionsDeladem EmmanuelNo ratings yet
- Adverse Effects: Blood TransfusionDocument43 pagesAdverse Effects: Blood TransfusionDumindu PereraNo ratings yet
- Blood Transfusion Complications & Management (40Document30 pagesBlood Transfusion Complications & Management (40kushalNo ratings yet
- Division of Blood Transfusion Services: Ministry of Health and Family WelfareDocument46 pagesDivision of Blood Transfusion Services: Ministry of Health and Family WelfareKirandragonNo ratings yet
- Blood Transfusion Reaction 3032018Document33 pagesBlood Transfusion Reaction 3032018Kelly YeowNo ratings yet
- Transfusion Medicine by Dr. Sharad JohriDocument54 pagesTransfusion Medicine by Dr. Sharad JohriShashwat JohriNo ratings yet
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- Lecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiDocument41 pagesLecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiMudassar Roomi100% (1)
- ICU Blood Transfusion & Electrolytes DisturbanceDocument26 pagesICU Blood Transfusion & Electrolytes Disturbancef6080683No ratings yet
- Adverse Effects of Plasma TherapyDocument80 pagesAdverse Effects of Plasma TherapyShaiji ShahidNo ratings yet
- A-Gvhd M.saeedDocument20 pagesA-Gvhd M.saeedaymenNo ratings yet
- Unit - 5 Blood Banking HaematologyDocument82 pagesUnit - 5 Blood Banking HaematologySumit PandyaNo ratings yet
- Hematology Transfusion ReactionDocument69 pagesHematology Transfusion ReactionSharmin Nahar NabilaNo ratings yet
- Blood Transfusion ReactionsDocument8 pagesBlood Transfusion ReactionsStephanie AngelaNo ratings yet
- Blood Transfusion Basic Concepts Blood Transfusion inDocument103 pagesBlood Transfusion Basic Concepts Blood Transfusion iniahmad9No ratings yet
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsAulia RahmanNo ratings yet
- Rules of TransfusionDocument4 pagesRules of Transfusionapi-233414716100% (1)
- Session 8Document6 pagesSession 8madcalNo ratings yet
- 7 Adverse Reactions to TransfusionDocument11 pages7 Adverse Reactions to TransfusiondrkamalakarNo ratings yet
- Hemolytic Disease of the Fetus and Newborn (HDFNDocument46 pagesHemolytic Disease of the Fetus and Newborn (HDFNK.M.S. ChathunikaNo ratings yet
- Transfusion of Blood and Red CellsDocument34 pagesTransfusion of Blood and Red CellsAdams Westlifer SophianoNo ratings yet
- ITP LectureDocument20 pagesITP LectureReza MajidiNo ratings yet
- 145 278 1 SMDocument28 pages145 278 1 SMAtika RosmiaNo ratings yet
- 5 Transfusion ReactionsDocument34 pages5 Transfusion ReactionsFuentes, Jade Andrey R. BSMT 2-ANo ratings yet
- Blood & Blood ProductsDocument29 pagesBlood & Blood Productsneelam aliNo ratings yet
- Blood Transfusion Blood Grouping and Cross MatchingDocument46 pagesBlood Transfusion Blood Grouping and Cross MatchingHa LeemNo ratings yet
- 11a. Blood TransfusionDocument28 pages11a. Blood TransfusionMuwanga faizoNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic DisorderZoe DorothyNo ratings yet
- Surgery Slide 6 - Blood TransfusionsDocument54 pagesSurgery Slide 6 - Blood TransfusionsEman NazzalNo ratings yet
- Blood Transfusion 2Document12 pagesBlood Transfusion 2Helene AlawamiNo ratings yet
- Transfusion Medicine: DR Abdullah AnsariDocument53 pagesTransfusion Medicine: DR Abdullah AnsariFabsNo ratings yet
- Essential principles and complications of blood transfusionDocument27 pagesEssential principles and complications of blood transfusionisuhuNo ratings yet
- Blood Transfusion Notes..Document9 pagesBlood Transfusion Notes..queenethNo ratings yet
- Blood transfusionDocument20 pagesBlood transfusionGladys OdibuNo ratings yet
- Local Media4202655613631600684Document6 pagesLocal Media4202655613631600684Haniya KhanNo ratings yet
- Pediatric Transfusion Risks and GuidelinesDocument57 pagesPediatric Transfusion Risks and GuidelinesDR.RAJESWARI SUBRAMANIYANNo ratings yet
- Adverse Effects of Blood TransfusionDocument3 pagesAdverse Effects of Blood Transfusionay254No ratings yet
- Blood Transfusion Reactions: Life Saving Yet Life ThreateningDocument52 pagesBlood Transfusion Reactions: Life Saving Yet Life Threateninganam farzand100% (2)
- Blood TransfusionDocument58 pagesBlood Transfusionmsat72100% (12)
- Blood Transfusion Guide for Immediate ReactionsDocument8 pagesBlood Transfusion Guide for Immediate ReactionsJohann OrtizNo ratings yet
- Pediatric TransfusionDocument82 pagesPediatric TransfusionMia Lesaca-Medina100% (2)
- Research questions on blood typing procedures and hemolytic disease of the newborn (HDNDocument3 pagesResearch questions on blood typing procedures and hemolytic disease of the newborn (HDNBrielleNo ratings yet
- Transfusion RXNsDocument67 pagesTransfusion RXNsSuha Abdullah100% (1)
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument27 pagesHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanNo ratings yet
- Blood TransfusionDocument57 pagesBlood Transfusionibzshan_No ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Adverse Effects of TransfusionDocument5 pagesAdverse Effects of Transfusionlubna aloshibiNo ratings yet
- Adverse Effects of TransfusionDocument5 pagesAdverse Effects of Transfusionlubna aloshibiNo ratings yet
- Complications of Blood TransfusionDocument15 pagesComplications of Blood TransfusionAdeniran CharlesNo ratings yet
- Cardiovascular Pathology GuideDocument33 pagesCardiovascular Pathology GuideAdeniran CharlesNo ratings yet
- Anxiolytic and Hypnotic Drugs 2Document44 pagesAnxiolytic and Hypnotic Drugs 2Adeniran CharlesNo ratings yet
- 2020-2021 Practical and Tutorial ScheduleDocument5 pages2020-2021 Practical and Tutorial ScheduleAdeniran CharlesNo ratings yet
- Acute Renal Failure: Dr. Sami Abdo RadmanDocument23 pagesAcute Renal Failure: Dr. Sami Abdo RadmanAdeniran CharlesNo ratings yet
- Cell wall inhibitors cell wall dysfunction mechanismsDocument99 pagesCell wall inhibitors cell wall dysfunction mechanismsAdeniran CharlesNo ratings yet
- Principles of HIV TreatmentDocument67 pagesPrinciples of HIV TreatmentAdeniran CharlesNo ratings yet
- Protein synthesis inhibitor: Tetracyclines inhibit protein synthesisDocument113 pagesProtein synthesis inhibitor: Tetracyclines inhibit protein synthesisAdeniran CharlesNo ratings yet
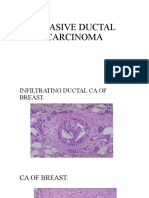
- Invasive Ductal CarcinomaDocument3 pagesInvasive Ductal CarcinomaAdeniran CharlesNo ratings yet
- Neuromuscular Pharmacology 305-1Document43 pagesNeuromuscular Pharmacology 305-1Adeniran CharlesNo ratings yet
- The Drawing WebsiteDocument99 pagesThe Drawing WebsiteAdeniran CharlesNo ratings yet
- Clinical Blood TransfusionDocument13 pagesClinical Blood TransfusionAdeniran CharlesNo ratings yet
- HAEMATOLOGIC MANIFESTATIONS OF SYSTEMIC DISEASESDocument38 pagesHAEMATOLOGIC MANIFESTATIONS OF SYSTEMIC DISEASESAdeniran CharlesNo ratings yet
- Burkitt's Lymphoma BbcockDocument27 pagesBurkitt's Lymphoma BbcockAdeniran CharlesNo ratings yet
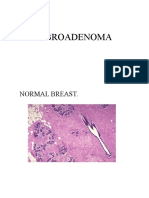
- Fi Bro AdenomaDocument4 pagesFi Bro AdenomaAdeniran CharlesNo ratings yet
- Administration of MedicationDocument18 pagesAdministration of MedicationThilaga RamNo ratings yet
- Chapter 5Document50 pagesChapter 5kebNo ratings yet
- Hoeltke Chapter5 RevisedDocument34 pagesHoeltke Chapter5 RevisedPrincess Weiyoung100% (1)
- ACOG Practice Bulletin No 75 Management of 44 1 PDFDocument8 pagesACOG Practice Bulletin No 75 Management of 44 1 PDFTanuj sai kumarNo ratings yet
- Blood Lecture SlidesDocument144 pagesBlood Lecture Slidesgrace ncubeNo ratings yet
- Blood DisordersDocument111 pagesBlood DisordersAbuzarNo ratings yet
- HaematopoiesisDocument4 pagesHaematopoiesisGerardLum100% (1)
- Pamflet Donor DarahDocument3 pagesPamflet Donor DarahAlifianti Balinda PramatasariNo ratings yet
- Anatomical structures in Cells at Work animeDocument3 pagesAnatomical structures in Cells at Work animeRochele ForondaNo ratings yet
- (MT 6318 LAB) Compiled 3rd Shifting TopicsDocument21 pages(MT 6318 LAB) Compiled 3rd Shifting Topicslanceferdinand.tan.pharmaNo ratings yet
- EPITHELIAL TISSUE (Epithelium / Epithelia) : Basement MembraneDocument7 pagesEPITHELIAL TISSUE (Epithelium / Epithelia) : Basement MembraneNanaNo ratings yet
- Different Types of TissueDocument6 pagesDifferent Types of TissueJamesMarcoM100% (1)
- Ch. 1 SummaryDocument2 pagesCh. 1 SummaryAnna GassettNo ratings yet
- Medical Laboratory Tests: Tang PingDocument42 pagesMedical Laboratory Tests: Tang Pingapi-19916399No ratings yet
- Plant Tissues Types and FunctionsDocument2 pagesPlant Tissues Types and FunctionsJames Carbonell Dela PeñaNo ratings yet
- Understanding Blood Collection TubesDocument47 pagesUnderstanding Blood Collection TubesMARK VINCENT BAUTISTANo ratings yet
- 4 Circulation Disorders PDFDocument69 pages4 Circulation Disorders PDFSetiawan SukmadjaNo ratings yet
- 32.2 Science Notebook SheetDocument3 pages32.2 Science Notebook SheetMaya KhaledNo ratings yet
- KampoloDocument26 pagesKampoloSalifyanji SimpambaNo ratings yet
- 7 5 16 Physiology of Red Blood CellsDocument72 pages7 5 16 Physiology of Red Blood CellsJoshua NyazonNo ratings yet
- Evaluation Tests For Secondary Hemostasis (Lab Analysis) HematologyDocument5 pagesEvaluation Tests For Secondary Hemostasis (Lab Analysis) HematologyAudreySlitNo ratings yet
- Muscles and Movements: Types of Muscles Structure of Skeletal MusclesDocument16 pagesMuscles and Movements: Types of Muscles Structure of Skeletal MusclesMahin FatimaNo ratings yet
- Animal Tissue Concept MapDocument1 pageAnimal Tissue Concept MapBeyonce C. SIBALNo ratings yet
- CBC PDFDocument1 pageCBC PDFEllen AquinoNo ratings yet
- Physiology, Lecture 5, Blood (Lecture Notes)Document10 pagesPhysiology, Lecture 5, Blood (Lecture Notes)Ali Al-Qudsi100% (1)
- BVBDocument23 pagesBVBIFOZANNo ratings yet
- Antibody Screening and IdentificationDocument13 pagesAntibody Screening and IdentificationAnonymouscatNo ratings yet
- Histology Note of Circulatory SystemDocument8 pagesHistology Note of Circulatory System陳碩璠No ratings yet
- HEMATOLOGY SECRETS FOR CATS & DOGSDocument88 pagesHEMATOLOGY SECRETS FOR CATS & DOGSŞtefania MafteiNo ratings yet