You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Theoretical Foundation of NursingDocument60 pagesTheoretical Foundation of NursingViea Pacaco Siva100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Form 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerDocument1 pageForm 2A. Laboratory Request and Result Form: To Be Filled Out by Health WorkerJuvy Micutuan100% (2)
- Dosha Gati NotesDocument5 pagesDosha Gati NotesbalatnNo ratings yet
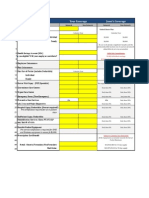
- Medical Benefits SummaryDocument1 pageMedical Benefits SummaryJanet Zimmerman McNicholNo ratings yet
- Case Presentation: Group 2Document30 pagesCase Presentation: Group 2Wendy EscalanteNo ratings yet
- Dental Assisting Course Work ReportDocument6 pagesDental Assisting Course Work Reportf5dmncxc100% (2)
- 06 Why Did You Decide To Be A DentistDocument10 pages06 Why Did You Decide To Be A Dentistangi paola puicon ruizNo ratings yet
- Survival GuideDocument4 pagesSurvival Guideeclipse1130No ratings yet
- Main EssayDocument7 pagesMain EssayKen UcheonyeNo ratings yet
- Adaptive ImmunityDocument6 pagesAdaptive ImmunityAvinash SahuNo ratings yet
- Drugs Acting On The Immune System: Retchel-Elly D. Dapli-AnDocument60 pagesDrugs Acting On The Immune System: Retchel-Elly D. Dapli-AnJoshua MendozaNo ratings yet
- NCM 119 Clinical MEDICINE WARD Activity 1 G3 BSN 4 2Document13 pagesNCM 119 Clinical MEDICINE WARD Activity 1 G3 BSN 4 2Allysa MacalinoNo ratings yet
- Imle 15.02.2016 PDFDocument70 pagesImle 15.02.2016 PDFRaZy Abo RayaNo ratings yet
- Inovasi Implementasi Puskesmas Poned Dalam Upaya A PDFDocument7 pagesInovasi Implementasi Puskesmas Poned Dalam Upaya A PDFSVJ officialNo ratings yet
- OHCEA Abstract Report PDFDocument123 pagesOHCEA Abstract Report PDFDenis Michael WamalaNo ratings yet
- CaballeroaDocument13 pagesCaballeroaapi-549069910No ratings yet
- Vas BerryDocument1 pageVas BerryNabaa AlhammadiNo ratings yet
- Cestosis y Cestodos PDFDocument14 pagesCestosis y Cestodos PDFErnesto VersailleNo ratings yet
- LSS GB SIPOC Diagram Johnson Anderson2Document2 pagesLSS GB SIPOC Diagram Johnson Anderson2Seda De DrasniaNo ratings yet
- Systemic Lupus ErythematosusDocument9 pagesSystemic Lupus ErythematosusTheeya QuigaoNo ratings yet
- Pep Certificate 1Document1 pagePep Certificate 1api-283487476No ratings yet
- W3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Document22 pagesW3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Rona DindangNo ratings yet
- Chapter 1 Developmental PsychopathologyDocument30 pagesChapter 1 Developmental PsychopathologyLAVANYA M PSYCHOLOGY-COUNSELLINGNo ratings yet
- Pe 1 CLPDocument15 pagesPe 1 CLPMary Rose FalconeNo ratings yet
- Abdominal Radical Trachelectomy: A Romanian SeriesDocument5 pagesAbdominal Radical Trachelectomy: A Romanian SeriesPanuta AndrianNo ratings yet
- Behçet DiseaseDocument17 pagesBehçet DiseasePaolo QuezonNo ratings yet
- BOS Mini ScrewsDocument2 pagesBOS Mini ScrewsWajeeha YounisNo ratings yet
- Study PlanDocument9 pagesStudy PlanHNo ratings yet
- Jamia Hamdard Hamdard Nagar, New Delhi: Application Form For Non-Academic and Technical PostsDocument5 pagesJamia Hamdard Hamdard Nagar, New Delhi: Application Form For Non-Academic and Technical PostsAnonymous e8SuLivNo ratings yet
- Decubitus Ulcer Wound Care - RefratDocument35 pagesDecubitus Ulcer Wound Care - RefratheraNo ratings yet