You might also like
- Jurnal Coronary Artery FistulaDocument3 pagesJurnal Coronary Artery FistulaRistinyaUnuyNo ratings yet
- Echo Case Ao RegurgDocument3 pagesEcho Case Ao Regurgdgina8800No ratings yet
- Icrj 04 94Document3 pagesIcrj 04 94Bogdan-Marian DragoescuNo ratings yet
- Coronary Sinus Aneurysm: Incidental Discovery During Coronary Artery Bypass GraftingDocument3 pagesCoronary Sinus Aneurysm: Incidental Discovery During Coronary Artery Bypass GraftingasclepiuspdfsNo ratings yet
- Atrial Hemangioma A Case Report and Review of The LiteratureDocument11 pagesAtrial Hemangioma A Case Report and Review of The LiteratureSaya MenarikNo ratings yet
- ArtigosDocument6 pagesArtigosIgor PiresNo ratings yet
- Kardo S 1998Document3 pagesKardo S 1998Sarly FebrianaNo ratings yet
- Omar 2014Document5 pagesOmar 2014Fede WeckesserNo ratings yet
- Best Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsDocument7 pagesBest Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsReinaldi octaNo ratings yet
- Aranda 1998Document5 pagesAranda 1998Sarly FebrianaNo ratings yet
- Cardiac LipomDocument4 pagesCardiac LipomCiprian MarianNo ratings yet
- Presentacion Hoja de Papel Creativa RosadoDocument26 pagesPresentacion Hoja de Papel Creativa Rosadoapi-702934667No ratings yet
- Jurnal Giant Pericardial CystDocument4 pagesJurnal Giant Pericardial CystJicko Street HooligansNo ratings yet
- Right Coronary Artery-Right Atrial Fistula in Right Atrial Myxoma A Rare CombinationDocument3 pagesRight Coronary Artery-Right Atrial Fistula in Right Atrial Myxoma A Rare CombinationAxel Hiram Hernandez PinedaNo ratings yet
- Tortuosity,: Coiling, and Kinking of Internal Carotid ArteryDocument13 pagesTortuosity,: Coiling, and Kinking of Internal Carotid ArteryRoberto AmayaNo ratings yet
- Ghaffarian2018 PDFDocument4 pagesGhaffarian2018 PDFIgor PiresNo ratings yet
- Clinical Cases: Ischaemic Heart DiseaseDocument4 pagesClinical Cases: Ischaemic Heart DiseaseLADY JOWAHER ALLASNo ratings yet
- Pathology Report - Nisal KarawitaDocument7 pagesPathology Report - Nisal KarawitaNisal KarawitaNo ratings yet
- Anatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicDocument5 pagesAnatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicFarida FaradillaNo ratings yet
- Circulation 1973 ALONSO 588 96Document10 pagesCirculation 1973 ALONSO 588 96Jessica ARNo ratings yet
- Abstract Submision Fo Wecoc 2023Document2 pagesAbstract Submision Fo Wecoc 2023Egi Dwi SatriaNo ratings yet
- Shaabi2014 PDFDocument3 pagesShaabi2014 PDFIgor PiresNo ratings yet
- Coronary Angiographic Morphology in Myocardial Infarction: A Link Between The Pathogenesis of Unstable Angina and Myocardial InfarctionDocument6 pagesCoronary Angiographic Morphology in Myocardial Infarction: A Link Between The Pathogenesis of Unstable Angina and Myocardial InfarctionSabila RosyidaNo ratings yet
- 1 s2.0 S2468644123001299 MainDocument6 pages1 s2.0 S2468644123001299 MainRonald QuezadaNo ratings yet
- 10.1007@s00296 008 0601 0Document3 pages10.1007@s00296 008 0601 0Kuber RawaNo ratings yet
- Percutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial InfarctionDocument4 pagesPercutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial Infarctionvam buddhaNo ratings yet
- CLC 23 149Document6 pagesCLC 23 149Kahina AmroucheNo ratings yet
- Diagnosis of Double-Chambered Left Ventricle by Contrast Echocardiography: A Case ReportDocument6 pagesDiagnosis of Double-Chambered Left Ventricle by Contrast Echocardiography: A Case ReportMasithaNo ratings yet
- Adult Choroidal Vein of Galen MalformationDocument5 pagesAdult Choroidal Vein of Galen MalformationSonia Prima Arisa PutriNo ratings yet
- cazuriDocument4 pagescazuriIbănescu Iulia AndreeaNo ratings yet
- Pi Is 0003497516313285Document3 pagesPi Is 0003497516313285Gordana PuzovicNo ratings yet
- Criss-Cross Heart With Double-Outlet Right VentricleDocument4 pagesCriss-Cross Heart With Double-Outlet Right Ventriclejuana lopezNo ratings yet
- Treating Giant AVM and Aneurysm Rupture During PregnancyDocument4 pagesTreating Giant AVM and Aneurysm Rupture During PregnancymutiahmuftihNo ratings yet
- Coronary Arteri DiseaseDocument3 pagesCoronary Arteri DiseasetriNo ratings yet
- Giant Coronary Artery Aneurysms in Kawasaki Disease Detected by Multi Detector Computed TomographicDocument3 pagesGiant Coronary Artery Aneurysms in Kawasaki Disease Detected by Multi Detector Computed TomographicVigoNo ratings yet
- Dca RahulDocument72 pagesDca RahulyuliaNo ratings yet
- Transhepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDocument3 pagesTranshepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDavids MarinNo ratings yet
- Particularities of Scimitar Syndrome in Adult PatientsDocument5 pagesParticularities of Scimitar Syndrome in Adult PatientsIJAR JOURNALNo ratings yet
- CT Shows Diffuse Fatty Thickening of Interatrial SeptumDocument13 pagesCT Shows Diffuse Fatty Thickening of Interatrial SeptumHaluk AlibazogluNo ratings yet
- Anomalous Coronary ArteriesDocument7 pagesAnomalous Coronary ArteriesYonatan Merchant PerezNo ratings yet
- Giant Left Atrial Appendage Aneurysm and Right Ventricular Diverticulum: A Very Rare AssociationDocument4 pagesGiant Left Atrial Appendage Aneurysm and Right Ventricular Diverticulum: A Very Rare AssociationIJAR JOURNALNo ratings yet
- A Complete LBBB Revealing Non Specific Venous Metastasis Into The Right Atrium: A Case Report and Review of LiteratureDocument7 pagesA Complete LBBB Revealing Non Specific Venous Metastasis Into The Right Atrium: A Case Report and Review of LiteratureIJAR JOURNALNo ratings yet
- Taniguchi 2007Document3 pagesTaniguchi 2007Kuber RawaNo ratings yet
- 856 t2sv87Document6 pages856 t2sv87AntonisNo ratings yet
- Carotid Artery Stenosis ImagingDocument10 pagesCarotid Artery Stenosis ImagingCristhian RuizNo ratings yet
- Left Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationDocument3 pagesLeft Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationIsabella María GantivarNo ratings yet
- Echographie Cardiaque AnglaisDocument1 pageEchographie Cardiaque AnglaiswkoussahNo ratings yet
- Anomalous Origin of The Coronary Artery From The Pulmonary Artery in Children and Adults - A Pictorial Review of Cardiac Imaging FindingsDocument10 pagesAnomalous Origin of The Coronary Artery From The Pulmonary Artery in Children and Adults - A Pictorial Review of Cardiac Imaging FindingsChici FarlinaNo ratings yet
- Acute Myocardial Infarction en Estenosis Aortica Severa Con Coronarias NormalesDocument4 pagesAcute Myocardial Infarction en Estenosis Aortica Severa Con Coronarias NormalesfabiandionisioNo ratings yet
- C P P C P P: Ardiology Atient AGE Ardiology Atient AGEDocument4 pagesC P P C P P: Ardiology Atient AGE Ardiology Atient AGEsatish_vsNo ratings yet
- Isolated Right Ventricle Myocardial Infarction - Is The Right Ventricle Still The Forgotten Ventricle?Document4 pagesIsolated Right Ventricle Myocardial Infarction - Is The Right Ventricle Still The Forgotten Ventricle?Nadyaindriati96No ratings yet
- Obstructed Mediastinal Venous Flow Reverses Brain ScanDocument4 pagesObstructed Mediastinal Venous Flow Reverses Brain ScanRia AngganiNo ratings yet
- Iatrogenic Acute Aortic Dissection during PPCIDocument4 pagesIatrogenic Acute Aortic Dissection during PPCISajjad HussainNo ratings yet
- 2013 Adjustment of The Surgical Plan in Repair of Congenital Heart Disease - The Power of Cross-Sectional Imaging and Three-Dimensional VisualizationDocument6 pages2013 Adjustment of The Surgical Plan in Repair of Congenital Heart Disease - The Power of Cross-Sectional Imaging and Three-Dimensional Visualizationccvped3dNo ratings yet
- Medicine: DR: Jawad 9-Oct-06 Lec: - 3Document3 pagesMedicine: DR: Jawad 9-Oct-06 Lec: - 3api-3829364No ratings yet
- Mca 8699Document3 pagesMca 8699mohdmuntazahmedNo ratings yet
- 43 B 625754151 Facf 91 EcDocument25 pages43 B 625754151 Facf 91 Ecapi-702934667No ratings yet
- Noncompaction of The Left Ventricle in A Patient With DextroversionDocument4 pagesNoncompaction of The Left Ventricle in A Patient With DextroversionDinda Wanodya SNo ratings yet
- Cerebellar Venous Infarction in Chronic Suppurative Otitis MediaDocument4 pagesCerebellar Venous Infarction in Chronic Suppurative Otitis MediamuhammadNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
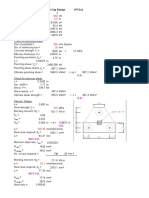
- Check For Punching Shear:: Pile Cap Design (PC3a)Document4 pagesCheck For Punching Shear:: Pile Cap Design (PC3a)Sheikh Mizanur RahmanNo ratings yet
- Check For Punching Shear:: Pile Cap Design (PC3a)Document6 pagesCheck For Punching Shear:: Pile Cap Design (PC3a)Sheikh Mizanur RahmanNo ratings yet
- Section DesignerDocument191 pagesSection DesignergreatwellwisherNo ratings yet
- Training DisclaimerDocument2 pagesTraining DisclaimermihaitimofteNo ratings yet
- Newhope Silo Budget FormDocument1 pageNewhope Silo Budget FormSheikh Mizanur RahmanNo ratings yet
- Keyboard shortcuts for Tekla StructuresDocument2 pagesKeyboard shortcuts for Tekla StructuresUmt KcNo ratings yet
- Septic Tank Design Program RAS2021 Updated 10.8.2009Document12 pagesSeptic Tank Design Program RAS2021 Updated 10.8.2009Sheikh Mizanur RahmanNo ratings yet
- 2 PC CirDocument4 pages2 PC CirSheikh Mizanur RahmanNo ratings yet
- Pile Cap of Footing F1Document4 pagesPile Cap of Footing F1Sheikh Mizanur RahmanNo ratings yet
- Butterworth - Finite Element Analysis of Structural Steelwork Beam To Column Bolted ConnectionsDocument14 pagesButterworth - Finite Element Analysis of Structural Steelwork Beam To Column Bolted ConnectionsLuis BarboNo ratings yet
- Civl432 Bridge Design SummaryDocument5 pagesCivl432 Bridge Design SummarySheikh Mizanur RahmanNo ratings yet
- Arch 220 - Steel Frame ConstructionDocument9 pagesArch 220 - Steel Frame ConstructionSheikh Mizanur RahmanNo ratings yet
- Tekla - Steel Detailing - Basic Training DrawingDocument160 pagesTekla - Steel Detailing - Basic Training DrawingEileen Christopher100% (1)
- Lesson14 ProjectManagerDocument46 pagesLesson14 ProjectManagercoolhunk80No ratings yet
- Tekla Custom Components For Steel 12Document29 pagesTekla Custom Components For Steel 12dorel1900No ratings yet
- Tekla - Full Detailing-Basic Training ModelingDocument1,362 pagesTekla - Full Detailing-Basic Training ModelingYoung Jekal92% (37)
- Tekla - Custom Component EditingDocument75 pagesTekla - Custom Component EditingYoyok Abi Kuswardoyo100% (2)
- Tekla - Standard DocumentsDocument530 pagesTekla - Standard DocumentsDemçe FlorjanNo ratings yet
- Tekla - Advanced FunctionsDocument90 pagesTekla - Advanced Functionsphearomsl100% (4)
- How To Adjust A NotchDocument4 pagesHow To Adjust A NotchSheikh Mizanur RahmanNo ratings yet
- How the main axis of a contour plate is determinedDocument2 pagesHow the main axis of a contour plate is determinedSheikh Mizanur RahmanNo ratings yet
- Custom Elements Basics PDFDocument5 pagesCustom Elements Basics PDFSheikh Mizanur RahmanNo ratings yet
- Lesson 07 AppliedSteelDetailingDocument48 pagesLesson 07 AppliedSteelDetailingnifty25No ratings yet
- Create A Custom PartDocument6 pagesCreate A Custom PartLambourghiniNo ratings yet
- Lesson11 CastUnitDrawing PDFDocument23 pagesLesson11 CastUnitDrawing PDFKadutrisampaNo ratings yet
- Lesson 03 InteractiveDetailing PrecastDocument46 pagesLesson 03 InteractiveDetailing PrecastBurgheleaGeorge0% (1)
- Creating PDF Documents From X SteelDocument8 pagesCreating PDF Documents From X SteelSheikh Mizanur RahmanNo ratings yet
- Tekla Structure - Lesson 08 - NumberingAndReports2Document23 pagesTekla Structure - Lesson 08 - NumberingAndReports2Kresno N SoetomoNo ratings yet
- Lesson 06 Profiles and MaterialsDocument25 pagesLesson 06 Profiles and MaterialsSourav HaitNo ratings yet
- Lesson4 CustomComponents Precast PDFDocument28 pagesLesson4 CustomComponents Precast PDFKadutrisampaNo ratings yet
- URAPIDILDocument41 pagesURAPIDILFrancesco LucianiNo ratings yet
- Pulmonary AngiographyDocument3 pagesPulmonary AngiographyBiway RegalaNo ratings yet
- Blood Pressure - Blood Pressure ChartDocument3 pagesBlood Pressure - Blood Pressure ChartMahmoud MaherNo ratings yet
- Diabetic Macrovascular DiseaseDocument31 pagesDiabetic Macrovascular DiseaseArina ChifulescuNo ratings yet
- Anatomy - Physiology (Chapter 12 - Heart)Document20 pagesAnatomy - Physiology (Chapter 12 - Heart)Avi ZychNo ratings yet
- Health Assessment - Cardiac & PVSDocument56 pagesHealth Assessment - Cardiac & PVSclaire3230No ratings yet
- Anatomy, Coverings, Walls of HeartDocument8 pagesAnatomy, Coverings, Walls of HeartDeniebev'z OrillosNo ratings yet
- The Heart LA WorksheetDocument4 pagesThe Heart LA Worksheeteas grade04No ratings yet
- Congenital Heart DefectsDocument13 pagesCongenital Heart DefectsGheluzee Herrera100% (2)
- Herbesser Injection LeafletDocument7 pagesHerbesser Injection LeafletLyaNo ratings yet
- Compare and Contrast Process in Plants and AnimalsDocument8 pagesCompare and Contrast Process in Plants and AnimalsKimberly EamilaoNo ratings yet
- Riyadh Ali 4/9/12 MDSC3311Document6 pagesRiyadh Ali 4/9/12 MDSC3311Hugh JacobsNo ratings yet
- 5 Body Fluids and Circulation: SolutionsDocument13 pages5 Body Fluids and Circulation: SolutionsEkta ManglaniNo ratings yet
- High Blood Pressure Is A Common Condition That Affects The BodyDocument7 pagesHigh Blood Pressure Is A Common Condition That Affects The BodyMc inloveNo ratings yet
- BRAIN AneurysmDocument14 pagesBRAIN AneurysmRikizu HobbiesNo ratings yet
- Cues Nursing Diagnosis Objectives Nursing Interventions Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Objectives Nursing Interventions Rationale EvaluationHarvey Lampa SelimNo ratings yet
- Acute Myocard InfarctDocument43 pagesAcute Myocard InfarctFiannisa SuNo ratings yet
- Lecture 1 ScalpDocument5 pagesLecture 1 Scalpnatheer ayedNo ratings yet
- Cardiovascular Medicine:Question 1Document101 pagesCardiovascular Medicine:Question 1abdullahmushlihNo ratings yet
- Lymphoid System Organs and Cells ExplainedDocument31 pagesLymphoid System Organs and Cells ExplainedMace DueñasNo ratings yet
- Product Monograph of TelmisartanDocument8 pagesProduct Monograph of Telmisartandini hanifaNo ratings yet
- Lab Manual - Human Heart - A+p - StudentDocument24 pagesLab Manual - Human Heart - A+p - Studentsyl0% (1)
- Starling ResistorDocument4 pagesStarling ResistornisargNo ratings yet
- Cardiomyopathy: Causes, Types and TreatmentDocument98 pagesCardiomyopathy: Causes, Types and TreatmentZellanien hdNo ratings yet
- Eficacia Del FlowaveDocument6 pagesEficacia Del FlowaveLISFLOWERNo ratings yet
- Dynamic Hemodynamic Monitoring Assesses Cardiovascular SufficiencyDocument23 pagesDynamic Hemodynamic Monitoring Assesses Cardiovascular SufficiencyJuan CarrascoNo ratings yet
- Pathophysiology of Hypertension: RAAS Activation and Organ DamageDocument2 pagesPathophysiology of Hypertension: RAAS Activation and Organ DamageAlvin RamirezNo ratings yet
- Function and Importance of The Cardiovascular SystemDocument3 pagesFunction and Importance of The Cardiovascular SystemBenjamin SmithNo ratings yet
- 2018 Oligemia, Penumbra, Infarction. Understanding Hypoperfusion With NeuroimagingDocument11 pages2018 Oligemia, Penumbra, Infarction. Understanding Hypoperfusion With NeuroimagingTote Cifuentes AmigoNo ratings yet
- CV CannulationDocument15 pagesCV CannulationDatta BedkkirNo ratings yet