You might also like
- Best Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsDocument7 pagesBest Management in Isolated Right Ventricular Hypoplasia With Septal Defects in AdultsReinaldi octaNo ratings yet
- Echo Case Ao RegurgDocument3 pagesEcho Case Ao Regurgdgina8800No ratings yet
- Anatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicDocument5 pagesAnatomic Correction of Transposition of The Great Arteries: A S A Result of Mustard's Report, The HemodynamicFarida FaradillaNo ratings yet
- Noncompaction of The Left Ventricle in A Patient With DextroversionDocument4 pagesNoncompaction of The Left Ventricle in A Patient With DextroversionDinda Wanodya SNo ratings yet
- Left Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationDocument3 pagesLeft Ventricular Diverticulum in Association With Bicuspid Aortic Valve and Pseudocoarctation: Hitherto Unreported AssociationIsabella María GantivarNo ratings yet
- 16 Chiari NetworkDocument3 pages16 Chiari NetworkHani NguyenNo ratings yet
- Journal of Arrhythmia: Case ReportDocument2 pagesJournal of Arrhythmia: Case ReportMusafa WidagdoNo ratings yet
- Omar 2014Document5 pagesOmar 2014Fede WeckesserNo ratings yet
- Aranda 1998Document5 pagesAranda 1998Sarly FebrianaNo ratings yet
- AR Yang Komplikasi Menjadi Gagal Jantung PDFDocument5 pagesAR Yang Komplikasi Menjadi Gagal Jantung PDFFitriani AlawiyahNo ratings yet
- Physiology Congenital: of DiseaseDocument5 pagesPhysiology Congenital: of DiseaseFirah Triple'sNo ratings yet
- Arun Case CircDocument3 pagesArun Case CircDavin TakaryantoNo ratings yet
- Ebsteins Anomaly-An OverviewDocument36 pagesEbsteins Anomaly-An OverviewRJMNo ratings yet
- Anatomical and Pathophysiological Classification of Congenital Heart DiseaseDocument16 pagesAnatomical and Pathophysiological Classification of Congenital Heart DiseasePietro PensoNo ratings yet
- Particularities of Scimitar Syndrome in Adult PatientsDocument5 pagesParticularities of Scimitar Syndrome in Adult PatientsIJAR JOURNALNo ratings yet
- Kardo S 1998Document3 pagesKardo S 1998Sarly FebrianaNo ratings yet
- Arteriovenous Fistula Between Descending Aorta and Left Inferior Pulmonary VeinDocument2 pagesArteriovenous Fistula Between Descending Aorta and Left Inferior Pulmonary VeinDavin TakaryantoNo ratings yet
- Xrayand ElectrocardiogramDocument104 pagesXrayand ElectrocardiogramdrelvNo ratings yet
- Case Reports: Aberrant Right Subclavian Artery Associated With A Common Origin of Carotid ArteriesDocument4 pagesCase Reports: Aberrant Right Subclavian Artery Associated With A Common Origin of Carotid ArteriesIrai MartínezNo ratings yet
- Clinical Cases: Ischaemic Heart DiseaseDocument4 pagesClinical Cases: Ischaemic Heart DiseaseLADY JOWAHER ALLASNo ratings yet
- Diag Imagem Shunt PDFDocument5 pagesDiag Imagem Shunt PDFIzabela RodriguesNo ratings yet
- Idiopathic Fascicular Left Ventricular Tachycardia: Linear Ablation Lesion Strategy For Noninducible or Nonsustained TachycardiaDocument6 pagesIdiopathic Fascicular Left Ventricular Tachycardia: Linear Ablation Lesion Strategy For Noninducible or Nonsustained TachycardiaRahmi SyuadzahNo ratings yet
- 53 Coronary Artery AnomaliesDocument5 pages53 Coronary Artery AnomaliesVictor PazNo ratings yet
- A Rare Case of PJRT Ablated On The Roof of The Left Atrium 2012Document4 pagesA Rare Case of PJRT Ablated On The Roof of The Left Atrium 2012Võ Từ NhấtNo ratings yet
- Diagnosis of Double-Chambered Left Ventricle by Contrast Echocardiography: A Case ReportDocument6 pagesDiagnosis of Double-Chambered Left Ventricle by Contrast Echocardiography: A Case ReportMasithaNo ratings yet
- Grossfeld 1997Document3 pagesGrossfeld 1997Ali AmokraneNo ratings yet
- Jurnal Coronary Artery FistulaDocument3 pagesJurnal Coronary Artery FistulaRistinyaUnuyNo ratings yet
- 1rabio (Oo'.: Proceedings MedicineDocument12 pages1rabio (Oo'.: Proceedings MedicineMadhumala KumariNo ratings yet
- Jurnal Giant Pericardial CystDocument4 pagesJurnal Giant Pericardial CystJicko Street HooligansNo ratings yet
- Vanson 1993Document8 pagesVanson 1993Vy Lê KhảNo ratings yet
- Intercoronary Communication Between The Circumflex and Right Coronary Arteries: A Very Rare Coronary AnomalyDocument2 pagesIntercoronary Communication Between The Circumflex and Right Coronary Arteries: A Very Rare Coronary AnomalyDANNA21No ratings yet
- Intraosseous Arteriovenous Malformations Mimicking Malignant DiseaseDocument7 pagesIntraosseous Arteriovenous Malformations Mimicking Malignant DiseaseNm SNo ratings yet
- Poster Situs InversusDocument1 pagePoster Situs InversusArum Ayu KartikaNo ratings yet
- KCJ 42 568Document3 pagesKCJ 42 568vam buddhaNo ratings yet
- Aortic Thrombus - Esophageal CancerDocument3 pagesAortic Thrombus - Esophageal CancerJayzel LaureanoNo ratings yet
- CLC 23 149Document6 pagesCLC 23 149Kahina AmroucheNo ratings yet
- Student Paper: Communication ÉtudianteDocument3 pagesStudent Paper: Communication ÉtudianteJohan DwiantokoNo ratings yet
- Jurding Transposition AortaDocument10 pagesJurding Transposition AortaSilmi Putri RahayuNo ratings yet
- Congenital Partial Right Pericardial Defect Associated With Herniation of The Right AtrialDocument3 pagesCongenital Partial Right Pericardial Defect Associated With Herniation of The Right Atrialcronoss21No ratings yet
- Situs Inversus Imaging - Practice Essentials, Radiography, Computed TomographyDocument9 pagesSitus Inversus Imaging - Practice Essentials, Radiography, Computed TomographyFadil DendiNo ratings yet
- Acute Aortic Syndrome – More in The SpectruDocument5 pagesAcute Aortic Syndrome – More in The Spectrufabiola shoshajNo ratings yet
- First Description of TVD in Basset HoundDocument4 pagesFirst Description of TVD in Basset HoundFlorencia SeneseNo ratings yet
- Nejmvcm 2004089Document7 pagesNejmvcm 2004089julian zuletaNo ratings yet
- SMJ-59-279Document5 pagesSMJ-59-279Faradiba MaricarNo ratings yet
- Double-Outlet Left Ventricle and Vascular MalformationsDocument3 pagesDouble-Outlet Left Ventricle and Vascular MalformationsRaul UrietaNo ratings yet
- Ghaffarian2018 PDFDocument4 pagesGhaffarian2018 PDFIgor PiresNo ratings yet
- Brainsci 10 00538Document12 pagesBrainsci 10 00538Charles MorrisonNo ratings yet
- Quadricuspid Aortic Valve and A Ventricular Septal Defect in A HorseDocument7 pagesQuadricuspid Aortic Valve and A Ventricular Septal Defect in A HorseJacob HaleNo ratings yet
- ArtigosDocument6 pagesArtigosIgor PiresNo ratings yet
- Decastro 1970Document4 pagesDecastro 1970myaqanithaNo ratings yet
- Ruptured Isolated Spinal Artery Aneurysms: Report of Two Cases and Review of The LiteratureDocument7 pagesRuptured Isolated Spinal Artery Aneurysms: Report of Two Cases and Review of The LiteratureArjang AhmadpourNo ratings yet
- cazuriDocument4 pagescazuriIbănescu Iulia AndreeaNo ratings yet
- Obstructed Mediastinal Venous Flow Reverses Brain ScanDocument4 pagesObstructed Mediastinal Venous Flow Reverses Brain ScanRia AngganiNo ratings yet
- Difficult Vascular Access Due to Rare Persistent Sciatic ArteryDocument2 pagesDifficult Vascular Access Due to Rare Persistent Sciatic ArteryOnur KNo ratings yet
- Letters To The Editor: Pulmonary Atresia With Intact Ventricular SeptumDocument2 pagesLetters To The Editor: Pulmonary Atresia With Intact Ventricular SeptumanindiawNo ratings yet
- 1958 CantrellDocument13 pages1958 CantrellAmro Al PeckNo ratings yet
- Transhepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDocument3 pagesTranshepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDavids MarinNo ratings yet
- Mitral Valve...Document4 pagesMitral Valve...ikbal rambalinoNo ratings yet
- BCR 2021 241644Document3 pagesBCR 2021 241644Davin TakaryantoNo ratings yet
- Fetal Cardiology: A Practical Approach to Diagnosis and ManagementFrom EverandFetal Cardiology: A Practical Approach to Diagnosis and ManagementNo ratings yet
- Week 13 - Digestive System Overveiw Flashcards QuizletDocument13 pagesWeek 13 - Digestive System Overveiw Flashcards QuizletMorgan ChristNo ratings yet
- Panca InderaDocument26 pagesPanca Inderakema_hiperkes100% (1)
- The Cardiovascular System: Elaine N. MariebDocument46 pagesThe Cardiovascular System: Elaine N. MariebIvann Chan MunarNo ratings yet
- PubertyDocument18 pagesPubertyNuhaYahyaNo ratings yet
- Polycystic Kidney DiseaseDocument13 pagesPolycystic Kidney DiseaseMadlen212No ratings yet
- Hypothyrodism in PregnancyDocument32 pagesHypothyrodism in Pregnancymohammed makki0% (1)
- Module 9 Lesson 4Document11 pagesModule 9 Lesson 4Faatoots FatsNo ratings yet
- CardiomegalyDocument91 pagesCardiomegalyMariquita Buenafe100% (1)
- Presentation JaundiceDocument49 pagesPresentation JaundiceVinoth KumarNo ratings yet
- Cape 2 Biology - Homeostasis &excretionDocument9 pagesCape 2 Biology - Homeostasis &excretionTamicka BonnickNo ratings yet
- Heart CH 12 PDFDocument65 pagesHeart CH 12 PDFGabriel Tafalla100% (1)
- Download Human Anatomy 6Th Edition Michael Mckinley full chapterDocument67 pagesDownload Human Anatomy 6Th Edition Michael Mckinley full chapterchristina.mcneil622100% (2)
- TSH blood testDocument1 pageTSH blood testtitilayo loveNo ratings yet
- Effects of MisalignmentsDocument1 pageEffects of Misalignmentsguillek1No ratings yet
- Human Anatomy Articles OverviewDocument9 pagesHuman Anatomy Articles OverviewMuhammad AliNo ratings yet
- ANPH 4114 PHAP 4114: Graduate School of MedicineDocument8 pagesANPH 4114 PHAP 4114: Graduate School of MedicinelovelysyafiqahNo ratings yet
- Red and White Blood Cell PostersDocument2 pagesRed and White Blood Cell Postersapi-169639475No ratings yet
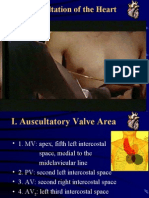
- Auscultation of HeartDocument92 pagesAuscultation of Heartsanjivdas100% (1)
- Tissue WorksheetDocument4 pagesTissue WorksheetFAITH ALBAÑEZNo ratings yet
- Endocrine System Multiple Choice QuestionsDocument42 pagesEndocrine System Multiple Choice QuestionswanderagroNo ratings yet
- Pathophysiology in Liver CirrhosisDocument4 pagesPathophysiology in Liver CirrhosisCyrus Ortalla RobinNo ratings yet
- Taste: Links in The Chain From Tongue To Brain: Lucy A. Vera and Stephen P. WoodingDocument6 pagesTaste: Links in The Chain From Tongue To Brain: Lucy A. Vera and Stephen P. WoodingCelzo RozaldoNo ratings yet
- Modelling Biological Neurons and Artificial Neural Networks (ANNDocument33 pagesModelling Biological Neurons and Artificial Neural Networks (ANNMary MorseNo ratings yet
- Neurotransmitter Release and ProcessDocument14 pagesNeurotransmitter Release and ProcessRain TolentinoNo ratings yet
- 1.introduction To Human BodyDocument16 pages1.introduction To Human BodyManjunathNo ratings yet
- Split-Brain Study Reveals Hemispheric SpecializationDocument1 pageSplit-Brain Study Reveals Hemispheric SpecializationAlisha GenduNo ratings yet
- Coordination & Response 3 QP PDFDocument10 pagesCoordination & Response 3 QP PDFJeffrey PiggottNo ratings yet
- Final Exam PracticeDocument6 pagesFinal Exam PracticeErvin T MileNo ratings yet
- Biology Nervous SystemDocument5 pagesBiology Nervous SystemFatima PueblaNo ratings yet
- Textbook Discussion On ST-elevation Myocardial Infarction - GicaroDocument12 pagesTextbook Discussion On ST-elevation Myocardial Infarction - GicaroJica Marie Bandiola GicaroNo ratings yet