You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Gas Turbine Compressor WashingDocument8 pagesGas Turbine Compressor Washingwolf_ns100% (1)
- Sample Paper III (Science) - Question PaperDocument21 pagesSample Paper III (Science) - Question Paperfathima MiranNo ratings yet
- Signal Integrity Modeling and Measurement of TSV in 3D ICDocument4 pagesSignal Integrity Modeling and Measurement of TSV in 3D IC張志榮No ratings yet
- Mathematics GR 11 Paper 2Document13 pagesMathematics GR 11 Paper 2ora mashaNo ratings yet
- Apl 220014Document2 pagesApl 220014Elprince MidoNo ratings yet
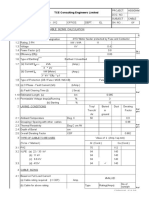
- Cable Sizing CalculationDocument72 pagesCable Sizing CalculationHARI my songs100% (1)
- C.KESAVAN - Diploma EEE: Phone No Mail IdDocument3 pagesC.KESAVAN - Diploma EEE: Phone No Mail IdKesavan ChinaswmiNo ratings yet
- Permutation PolynomialsDocument64 pagesPermutation Polynomialsmestrado unbNo ratings yet
- Creative Computing v06 n12 1980 DecemberDocument232 pagesCreative Computing v06 n12 1980 Decemberdarkstar314No ratings yet
- Substations - Part 1 - Procedural: DisclaimerDocument44 pagesSubstations - Part 1 - Procedural: DisclaimerSergio Henrique F. CArniettoNo ratings yet
- Dawn C. Meredith, Meaning MakingDocument2 pagesDawn C. Meredith, Meaning MakingMrsriyansyahNo ratings yet
- Open Source Software Development and Lotka's Law: Bibliometric Patterns in ProgrammingDocument10 pagesOpen Source Software Development and Lotka's Law: Bibliometric Patterns in ProgrammingAttya ShahidNo ratings yet
- CH 12 Review Solutions PDFDocument11 pagesCH 12 Review Solutions PDFOyinkansola OsiboduNo ratings yet
- Number Patterns and SequencesDocument10 pagesNumber Patterns and SequencesMohamed Hawash80% (5)
- 100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadDocument22 pages100 TOP Real Time Objective C Multiple Choice Questions and Answers PDF DownloadNayan BariNo ratings yet
- Presentation5 EV ArchitectureDocument26 pagesPresentation5 EV ArchitectureJAYKUMAR MUKESHBHAI THAKORNo ratings yet
- Newvhdl Syllabus (It&Cse)Document2 pagesNewvhdl Syllabus (It&Cse)Mude Kishore NaikNo ratings yet
- Kids Curriculum BreakdownDocument6 pagesKids Curriculum BreakdownSuniel ChhetriNo ratings yet
- OcrDocument16 pagesOcrBeena JaiswalNo ratings yet
- Circuit Protective Devices: Learner Work BookDocument41 pagesCircuit Protective Devices: Learner Work BookChanel Maglinao80% (5)
- Assignment 1Document2 pagesAssignment 1Alif Bukhari Imran NaimNo ratings yet
- Quantities Survey MethodsDocument73 pagesQuantities Survey MethodsparvezNo ratings yet
- Design of Helical Pier Foundations in Frozen GroundDocument6 pagesDesign of Helical Pier Foundations in Frozen GroundCortesar ManuNo ratings yet
- PPT5. SeptIITK - Crystal - Imperfections - DislocationsDocument92 pagesPPT5. SeptIITK - Crystal - Imperfections - DislocationsKartik Shankar KumbhareNo ratings yet
- Case StudyDocument10 pagesCase StudyVintage ArtNo ratings yet
- IFoA Directory of Actuarial Employers 2016-17-14102016Document22 pagesIFoA Directory of Actuarial Employers 2016-17-14102016Mian BialNo ratings yet
- DIO 1000 v1.1 - EN Op ManualDocument25 pagesDIO 1000 v1.1 - EN Op ManualMiguel Ángel Pérez FuentesNo ratings yet
- List of Knapsack Problems: 2 Multiple ConstraintsDocument3 pagesList of Knapsack Problems: 2 Multiple ConstraintssaiNo ratings yet
- Arithmetic Unit: Dr. Sowmya BJDocument146 pagesArithmetic Unit: Dr. Sowmya BJtinni09112003No ratings yet
- Triosonate in F (TWV 42-F7)Document17 pagesTriosonate in F (TWV 42-F7)EDMILSON BRUNO DO NASCIMENTONo ratings yet