You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Document4 pagesNUR 200 Tanner's Model - Noticing Through Reflecting-Updated 2020Oliver NamyaloNo ratings yet
- Terra Rosa E-Magazine No. 12Document33 pagesTerra Rosa E-Magazine No. 12Terra RosaNo ratings yet
- Child-Pugh Score & MELDDocument3 pagesChild-Pugh Score & MELDChaterine GraceNo ratings yet
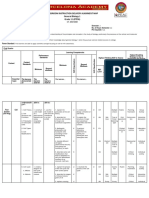
- Classroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)Document6 pagesClassroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)JunedelMirallesPerez50% (2)
- ISTSS Complex Trauma Treatment Guidelines 2012 Cloitre, Courtois, Ford, Green, Alexander, Briere, Herman, Lanius, Stolbach, Spinazzola, Van Der Kolk, Van Der HartDocument21 pagesISTSS Complex Trauma Treatment Guidelines 2012 Cloitre, Courtois, Ford, Green, Alexander, Briere, Herman, Lanius, Stolbach, Spinazzola, Van Der Kolk, Van Der HartSyifa Munawarah100% (1)
- 006 Pathology MCQ ACEM Primary CellularDocument5 pages006 Pathology MCQ ACEM Primary CellularIrum RafeeqNo ratings yet
- Professor Chamberlains 10 Rules of Normal ECGDocument12 pagesProfessor Chamberlains 10 Rules of Normal ECGAnusha Verghese83% (6)
- National Family Welfare ProgramDocument22 pagesNational Family Welfare ProgramAnuradha Maurya100% (9)
- Try Out Ujian Sekolah SMP Bahasa InggrisDocument23 pagesTry Out Ujian Sekolah SMP Bahasa InggrisGalih Setyo Sasongko100% (1)
- Proposa DAFPUS Awal Nian NianDocument4 pagesProposa DAFPUS Awal Nian NianAnia RandowichNo ratings yet
- Infographic Health and Well BeingDocument1 pageInfographic Health and Well BeingsomayaNo ratings yet
- RFID Chip will Poison Me and Kill me if I Disobey. Microchip Implants - RFID Brain Chip : Crime, Malpratice, Mindcontrol, Sexual Abuse, Brain Abuse, Torture Abuse, Medical Abuse, and The Silent Killers via RFID Brain ChipDocument3 pagesRFID Chip will Poison Me and Kill me if I Disobey. Microchip Implants - RFID Brain Chip : Crime, Malpratice, Mindcontrol, Sexual Abuse, Brain Abuse, Torture Abuse, Medical Abuse, and The Silent Killers via RFID Brain ChipJohanNo ratings yet
- CC2D KW Choy - Biochemical Testing in Acute and Chronic Kidney Failure PDFDocument40 pagesCC2D KW Choy - Biochemical Testing in Acute and Chronic Kidney Failure PDFSaad KhanNo ratings yet
- Ug Epidemiological Bulletin 2023Wk19Document8 pagesUg Epidemiological Bulletin 2023Wk19JACKLINE ONZIANo ratings yet
- Essentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankDocument25 pagesEssentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankNormanDanielsyftz100% (54)
- Defining A High-Performance lCU System For The - , 21st Century: A Position PaperDocument11 pagesDefining A High-Performance lCU System For The - , 21st Century: A Position PaperRodrigoSachiFreitasNo ratings yet
- Inguinal HernioplastyDocument10 pagesInguinal HernioplastyfiansisNo ratings yet
- Programme Abstracts Book 16052015Document297 pagesProgramme Abstracts Book 16052015wishfairy67100% (1)
- Composite Vs Amalgam PowerpointDocument17 pagesComposite Vs Amalgam Powerpointapi-322463366100% (1)
- Med Surg 1Document26 pagesMed Surg 1RogerQuxNo ratings yet
- E2language Test IDocument11 pagesE2language Test IBünyamin EmerNo ratings yet
- Industrialização TecnologicaDocument32 pagesIndustrialização TecnologicadanielreisNo ratings yet
- Tankersley Memo Pretrial Rel Bail ReformDocument37 pagesTankersley Memo Pretrial Rel Bail ReformCLDC_GSNo ratings yet
- Faculty of Veterinary Medicine: Academic GuidebookDocument13 pagesFaculty of Veterinary Medicine: Academic GuidebookAkbar FariNo ratings yet
- Harm Reduction: A British Columbia Community GuideDocument30 pagesHarm Reduction: A British Columbia Community GuideStephen OlsonNo ratings yet
- 2 Proposal NESTLE RevisedDocument8 pages2 Proposal NESTLE RevisedArif KamalNo ratings yet
- Southwestern University PHINMA School of Medicine Department of Medical Jurisprudence & Medical Ethics Medical Ethics and ProfessionalismDocument8 pagesSouthwestern University PHINMA School of Medicine Department of Medical Jurisprudence & Medical Ethics Medical Ethics and Professionalismthe urvashiNo ratings yet
- Nephrotic Syndrome (Nephrosis)Document9 pagesNephrotic Syndrome (Nephrosis)Madhusmita SatapathyNo ratings yet
- Normal Laboratory Values With Nursing Consideration - UsnganDocument8 pagesNormal Laboratory Values With Nursing Consideration - UsnganPrincess Nasima M. UsnganNo ratings yet
- Cert of Insur ExpandedDocument7 pagesCert of Insur Expandedmamie_rNo ratings yet