You might also like
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDocument3 pagesCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- PLAB Doable Subject Wise PDFDocument1,645 pagesPLAB Doable Subject Wise PDFAbdiNo ratings yet
- Quick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamDocument19 pagesQuick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamWyoXPat100% (11)
- Mnemonics for Medicine: Differential Diagnoses and Other PearlsFrom EverandMnemonics for Medicine: Differential Diagnoses and Other PearlsRating: 5 out of 5 stars5/5 (3)
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- Chronic Heart FailureDocument40 pagesChronic Heart FailureThea Concepcion100% (1)
- Supraventricular Arrhythmias GuideDocument17 pagesSupraventricular Arrhythmias GuideEdRobertArnadNo ratings yet
- ED Internal Medicine Oral Exam TopicsDocument10 pagesED Internal Medicine Oral Exam TopicsalirbidiNo ratings yet
- Alegrias Pat-FundsDocument14 pagesAlegrias Pat-Fundsapi-324006383No ratings yet
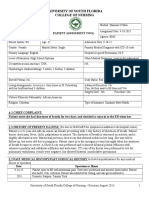
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument18 pagesUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-315731045No ratings yet
- Patient Assessment Tool ms2Document27 pagesPatient Assessment Tool ms2api-280998981No ratings yet
- ms2 Pat2Document22 pagesms2 Pat2api-315588288No ratings yet
- Pat 1 2015Document18 pagesPat 1 2015api-315192697No ratings yet
- Pat Ms IIDocument18 pagesPat Ms IIapi-339980385No ratings yet
- Pat FundamentalsDocument16 pagesPat Fundamentalsapi-339980385No ratings yet
- Pat 2 sd-1Document22 pagesPat 2 sd-1api-283672381No ratings yet
- Ms 1 PatDocument19 pagesMs 1 Patapi-281676750No ratings yet
- Pat Semester 1Document17 pagesPat Semester 1api-300946501No ratings yet
- Pat Msii November 2015Document20 pagesPat Msii November 2015api-301120253No ratings yet
- Pat 1 Medsurg 2Document18 pagesPat 1 Medsurg 2api-294300618No ratings yet
- Pat1 Med Surg 1Document19 pagesPat1 Med Surg 1api-339132978No ratings yet
- Pat Spring Ms II 2015Document16 pagesPat Spring Ms II 2015api-315435865No ratings yet
- Nur 4216 Pat 1 Med Surg 2 Noor TamariDocument18 pagesNur 4216 Pat 1 Med Surg 2 Noor Tamariapi-215323958No ratings yet
- Pat Revised 2013 1Document18 pagesPat Revised 2013 1api-324886317No ratings yet
- Pat Fall 2014Document21 pagesPat Fall 2014api-288536467No ratings yet
- ms1 PatDocument17 pagesms1 Patapi-325271731No ratings yet
- Pat 2 PortfolioDocument24 pagesPat 2 Portfolioapi-300861055No ratings yet
- Med Surg 2 Pat 1Document24 pagesMed Surg 2 Pat 1api-315444338No ratings yet
- Pat 2 Medsurg 2Document22 pagesPat 2 Medsurg 2api-315731045No ratings yet
- Pat Fall 2014Document17 pagesPat Fall 2014api-300849832No ratings yet
- Msii Pat 2Document22 pagesMsii Pat 2api-300946501No ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument20 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618No ratings yet
- Pat 2Document21 pagesPat 2api-270783686No ratings yet
- Pat 11052014Document18 pagesPat 11052014api-300362983No ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument17 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-340518534No ratings yet
- Pat 2 Med SurgDocument18 pagesPat 2 Med Surgapi-316861395No ratings yet
- Pat II MedsurgDocument19 pagesPat II Medsurgapi-301881424No ratings yet
- Pat DHDocument17 pagesPat DHapi-283153247No ratings yet
- ModMed CardiologyDocument77 pagesModMed CardiologyLee Tzong YewNo ratings yet
- Portfolio Pat 3Document19 pagesPortfolio Pat 3api-300861055No ratings yet
- Analisis Drug Related Problem (DRP) Pada Pasien Yang Terdiagnosa Gagal Ginjal Kronis Di Unit Rawat Inap Dahlia Rumah Sakit DR SuyotoDocument8 pagesAnalisis Drug Related Problem (DRP) Pada Pasien Yang Terdiagnosa Gagal Ginjal Kronis Di Unit Rawat Inap Dahlia Rumah Sakit DR Suyotodarmawan jsNo ratings yet
- Graded Pat 3Document10 pagesGraded Pat 3api-252750576No ratings yet
- Preassignment Work-Careplan #2Document30 pagesPreassignment Work-Careplan #2djbhetaNo ratings yet
- Pat Med Surg 1Document22 pagesPat Med Surg 1api-324658071No ratings yet
- Drug Study MahalDocument7 pagesDrug Study MahalBrylle ArbasNo ratings yet
- Final PatDocument22 pagesFinal Patapi-259394980No ratings yet
- Pat Revised 2013 1Document23 pagesPat Revised 2013 1api-314062228No ratings yet
- Pat MsiiDocument21 pagesPat Msiiapi-324658071No ratings yet
- Spring Pat 2Document22 pagesSpring Pat 2api-241359111No ratings yet
- Pat 2 - Med SurgDocument21 pagesPat 2 - Med Surgapi-315731045No ratings yet
- Stopp Start ToolkitDocument22 pagesStopp Start ToolkitRifky IlhamiNo ratings yet
- Pat 2 Med Surg - Dean GradedDocument24 pagesPat 2 Med Surg - Dean Gradedapi-252790184No ratings yet
- IMhpncrisisDocument8 pagesIMhpncrisischaoNo ratings yet
- Nursing Care Process Case StudyDocument6 pagesNursing Care Process Case StudyEunice RosalesNo ratings yet
- Maffett Fundamentals Pat 2015Document16 pagesMaffett Fundamentals Pat 2015api-339784339No ratings yet
- Pat 2014Document20 pagesPat 2014api-324658071No ratings yet
- Pat Revised 9-2014 FundamentalsDocument17 pagesPat Revised 9-2014 Fundamentalsapi-300362033No ratings yet
- OetDocument5 pagesOetGina Victor100% (2)
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument22 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-300454618No ratings yet
- University of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient InformationDocument18 pagesUniversity of South Florida College of Nursing: Msi & Msii Patient Assessment Tool 1 Patient Informationapi-340518534No ratings yet
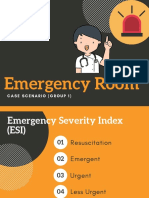
- Emergency Room: Case Scenario (Group 1)Document40 pagesEmergency Room: Case Scenario (Group 1)Victoria Castillo TamayoNo ratings yet
- Cardiac Failure Explained: Understanding the Symptoms, Signs, Medical Tests, and Management of a Failing HeartFrom EverandCardiac Failure Explained: Understanding the Symptoms, Signs, Medical Tests, and Management of a Failing HeartNo ratings yet
- Atrial Fibrillation Explained: Understanding The Next Cardiac EpidemicFrom EverandAtrial Fibrillation Explained: Understanding The Next Cardiac EpidemicNo ratings yet
- Alegrias Intro StatementDocument1 pageAlegrias Intro Statementapi-324006383No ratings yet
- Alegrias Personal GoalDocument1 pageAlegrias Personal Goalapi-324006383No ratings yet
- Alegrias Preceptorship EvalDocument1 pageAlegrias Preceptorship Evalapi-324006383No ratings yet
- Pat With Instructor FeedbackDocument19 pagesPat With Instructor Feedbackapi-324006383No ratings yet
- Alegrias Poster Nur 4634cDocument1 pageAlegrias Poster Nur 4634capi-324006383No ratings yet
- Alegrias TC CertificateDocument1 pageAlegrias TC Certificateapi-324006383No ratings yet
- Alegrias Synthesis PaperDocument11 pagesAlegrias Synthesis Paperapi-324006383No ratings yet
- Alegrias Community Health ImprovementDocument10 pagesAlegrias Community Health Improvementapi-324006383No ratings yet
- Alegrias CoverDocument1 pageAlegrias Coverapi-324006383No ratings yet
- Alegrias ResumeDocument2 pagesAlegrias Resumeapi-324006383No ratings yet
- Scientific Programme 18th APCC 090311Document33 pagesScientific Programme 18th APCC 090311drsmiNo ratings yet
- Heart RhythmsDocument68 pagesHeart Rhythmsyasahswi91No ratings yet
- J American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyDocument30 pagesJ American Geriatrics Society - 2023 - American Geriatrics Society 2023 Updated AGS Beers Criteria For PotentiallyOmyRojasNo ratings yet
- ABC of Clinical Electrocardiography Atrial ArrhythmiasDocument6 pagesABC of Clinical Electrocardiography Atrial ArrhythmiasIgnacio Aguilar ValdiviesoNo ratings yet
- Paag Esc Congress 2021Document14 pagesPaag Esc Congress 2021Carlos MlNo ratings yet
- Ecg Made EasyDocument343 pagesEcg Made EasyAbegail IbañezNo ratings yet
- Prescriber - 2020 - Barton - Classification and Choice of Antiarrhythmic TherapiesDocument7 pagesPrescriber - 2020 - Barton - Classification and Choice of Antiarrhythmic TherapiesCarlos Eduardo GómezNo ratings yet
- Catheter Ablationin in AF With CHFDocument11 pagesCatheter Ablationin in AF With CHFKristian Sudana HartantoNo ratings yet
- Journal Reading: Effects of Yoga in Patients With Paroxysmal Atrial Fibrillation - A Randomized Controlled StudyDocument50 pagesJournal Reading: Effects of Yoga in Patients With Paroxysmal Atrial Fibrillation - A Randomized Controlled StudyNovaria Puspita SamudraNo ratings yet
- Quick Reference GuideDocument2 pagesQuick Reference GuideHoàng Anh NguyễnNo ratings yet
- Hypertension in PregnancyDocument31 pagesHypertension in PregnancyradhabobbyNo ratings yet
- Arrhythmias Types, Pathophysiology AtfDocument9 pagesArrhythmias Types, Pathophysiology AtfAmir mohammad moori MohammadiNo ratings yet
- Exam 1 ER Chest PainDocument10 pagesExam 1 ER Chest Paindinkinspdd50% (2)
- Turkey Book 03 Internal Medicine PDFDocument47 pagesTurkey Book 03 Internal Medicine PDFPreaisNo ratings yet
- 1700 MCQ Revised VersionDocument485 pages1700 MCQ Revised VersionLu YaNo ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationireneaureliaNo ratings yet
- Medical Notes For Brian SlashDocument147 pagesMedical Notes For Brian SlashBrian Junwoo ParkNo ratings yet
- DR Erwin Sukandi, SPPD, K-KV BelumDocument47 pagesDR Erwin Sukandi, SPPD, K-KV BelumrajaalfatihNo ratings yet
- Message From The: Grand EastDocument50 pagesMessage From The: Grand EastglonyorgNo ratings yet
- Pediaatric Qs For GP Saudi Prometric PDFDocument84 pagesPediaatric Qs For GP Saudi Prometric PDFM A100% (2)
- ACLS Pre Course Package 2015 BC ActiveDocument40 pagesACLS Pre Course Package 2015 BC ActiverousbekNo ratings yet
- Cardio PDFDocument94 pagesCardio PDFSalwaNo ratings yet
- Administering Metoprolol IV Push 1Document22 pagesAdministering Metoprolol IV Push 1api-357388170No ratings yet
- ECG IntroDocument52 pagesECG IntroljgutierrezNo ratings yet
- Idea Pitching Apple Watch - CompressDocument6 pagesIdea Pitching Apple Watch - Compressabu40666No ratings yet