You might also like
- Squatting Will Decrease The Murmur in Mitral Valve Prolapse and Increase That of Hypertrophic Obstructive CardiomyopathyDocument15 pagesSquatting Will Decrease The Murmur in Mitral Valve Prolapse and Increase That of Hypertrophic Obstructive CardiomyopathyJoan ChoiNo ratings yet
- Evaluation PlanDocument64 pagesEvaluation PlanJoan ChoiNo ratings yet
- Russell Et Al-2011-The Cochrane Library - Sup-1Document3 pagesRussell Et Al-2011-The Cochrane Library - Sup-1Joan ChoiNo ratings yet
- The Effectiveness of Art Therapy Interventions in Reducing Post Traumatic Stress Disorder PTSD Symptoms in Pediatric Trauma PatientsDocument6 pagesThe Effectiveness of Art Therapy Interventions in Reducing Post Traumatic Stress Disorder PTSD Symptoms in Pediatric Trauma PatientsJoan Choi0% (1)
- Summary of Recommendations For Clinical Preventive Services: June 2016Document20 pagesSummary of Recommendations For Clinical Preventive Services: June 2016Joan ChoiNo ratings yet
- The Musculoskeletal System: Common Problems Ambulatory Care MedicineDocument116 pagesThe Musculoskeletal System: Common Problems Ambulatory Care MedicineJoan ChoiNo ratings yet
- Genetics: Duchenne Muscular Dystrophy (DMD) : Ages 2-5 W X-Recessive Gold Standard For DX: Genetic StudiesDocument1 pageGenetics: Duchenne Muscular Dystrophy (DMD) : Ages 2-5 W X-Recessive Gold Standard For DX: Genetic StudiesJoan ChoiNo ratings yet
- Initial Interview TemplateDocument4 pagesInitial Interview TemplateJoan ChoiNo ratings yet
- The Initial Psychiatric Interview PDFDocument4 pagesThe Initial Psychiatric Interview PDFJoan ChoiNo ratings yet
- Uworld Skin DisordersDocument5 pagesUworld Skin DisordersJoan ChoiNo ratings yet
- Mental Status ExamDocument2 pagesMental Status ExamJoan ChoiNo ratings yet
- Small WorldDocument88 pagesSmall WorldJoan ChoiNo ratings yet
- Uworld Peds MicroDocument5 pagesUworld Peds MicroJoan ChoiNo ratings yet
- The Basal Ganglia and Movement Disorders 2015 RevisedDocument19 pagesThe Basal Ganglia and Movement Disorders 2015 RevisedJoan ChoiNo ratings yet
- Psychiatry Shelf AnswersDocument8 pagesPsychiatry Shelf AnswersJoan Choi100% (1)
- Neurochemical Cascade of ConcussionDocument16 pagesNeurochemical Cascade of ConcussionJoan Choi100% (1)
- Sickle Cell PresentationDocument4 pagesSickle Cell PresentationJoan ChoiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Adelaide Uni Thesis SpecificationsDocument6 pagesAdelaide Uni Thesis Specificationslbbzfoxff100% (2)
- Soal Pas B.ing Peminatan Xii KirimDocument4 pagesSoal Pas B.ing Peminatan Xii KirimDavi DavioNo ratings yet
- Lakeshore BrochureDocument2 pagesLakeshore BrochurelakeshoreshoriansNo ratings yet
- Nihana Sherin P 11 16 2023 11 48 22 AMDocument2 pagesNihana Sherin P 11 16 2023 11 48 22 AMNihana sherinNo ratings yet
- Indian Council of Agricultural Research Krishi Anusandhan Bhawan-Ii, Pusa, New Delhi - 110 012Document7 pagesIndian Council of Agricultural Research Krishi Anusandhan Bhawan-Ii, Pusa, New Delhi - 110 012Bhupendra SinghNo ratings yet
- Weekly Lesson Plan Template Copy 2Document7 pagesWeekly Lesson Plan Template Copy 2api-357512470No ratings yet
- 02 - Case FormulationDocument18 pages02 - Case FormulationSanda Alina100% (4)
- Session No. 4/ Week No.4: Rizal Technological UniversityDocument12 pagesSession No. 4/ Week No.4: Rizal Technological UniversityKim FloresNo ratings yet
- 2023 Hoja Informativa FCE EXAM PRACTICE - FCP Ver.01Document2 pages2023 Hoja Informativa FCE EXAM PRACTICE - FCP Ver.01chavezinez7No ratings yet
- The Mental Capacity Act: Unit 305/HSC 036: Promote Person Centred Approaches in Health and Social CareDocument11 pagesThe Mental Capacity Act: Unit 305/HSC 036: Promote Person Centred Approaches in Health and Social CareJovana Ognenovska BakalovskaNo ratings yet
- Edid6512 Howell Design ProspectusDocument14 pagesEdid6512 Howell Design Prospectusapi-480904938No ratings yet
- One Month Study GuideDocument2 pagesOne Month Study GuideAshik Ishtiaque EmonNo ratings yet
- Lesson Plan Listening 1Document1 pageLesson Plan Listening 1Arlynne Zainal100% (3)
- Agaw Family (Kemant, Khamtanga, Qwarenya) : David Appleyard, SOASDocument3 pagesAgaw Family (Kemant, Khamtanga, Qwarenya) : David Appleyard, SOASKouame AdjepoleNo ratings yet
- Humanistic Learning Theory BastableDocument5 pagesHumanistic Learning Theory BastableNikki RicafrenteNo ratings yet
- Pgdba - Ob - 2022Document2 pagesPgdba - Ob - 2022arpan singhNo ratings yet
- Academic-Sccurriculumactionplan 2Document2 pagesAcademic-Sccurriculumactionplan 2api-392364749No ratings yet
- Mechanics of Deformable BodiesDocument8 pagesMechanics of Deformable BodiesCllyan ReyesNo ratings yet
- Wiki Fever - Catch It!: How Can Teachers Use Wikis To Facilitate Teaching and Learning?Document6 pagesWiki Fever - Catch It!: How Can Teachers Use Wikis To Facilitate Teaching and Learning?mdaniel2113No ratings yet
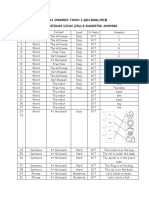
- Bahasa Inggeris Tahun 2 (Gg4 Mgbl/2018) Jadual Spesifikasi Ujian (Jsu) & Suggested AnswersDocument2 pagesBahasa Inggeris Tahun 2 (Gg4 Mgbl/2018) Jadual Spesifikasi Ujian (Jsu) & Suggested AnswersDayangku EffaNo ratings yet
- English 10 - 3rd Performance TaskDocument2 pagesEnglish 10 - 3rd Performance TaskDaa Karen Mae CocaNo ratings yet
- Factsheet RFL enDocument2 pagesFactsheet RFL enBhushan MulukNo ratings yet
- Literature Review s2 Handout PDFDocument23 pagesLiterature Review s2 Handout PDFFirsty MendrofaNo ratings yet
- Traditional Methods:: Ranking MethodDocument11 pagesTraditional Methods:: Ranking MethodSadhana Royal Athri PagadalaNo ratings yet
- Timetable MISSION 2024 Simplifying Your Preparation To Crack UPSC CSE 2024Document6 pagesTimetable MISSION 2024 Simplifying Your Preparation To Crack UPSC CSE 2024psthaakur097No ratings yet
- Reading Report in Reading in Philippine HistoryDocument8 pagesReading Report in Reading in Philippine HistoryChristine Jade MorenoNo ratings yet
- Alfarook Ziadeh - Personal StatementDocument2 pagesAlfarook Ziadeh - Personal Statementapi-719566584No ratings yet
- Form-12 KarenDocument2 pagesForm-12 KarenGeraldineMoletaGabutinNo ratings yet
- SNR Biology Syll Review ReportDocument10 pagesSNR Biology Syll Review ReportProHack RBXyoutubeNo ratings yet
- Fiesta SJMV 2019Document3 pagesFiesta SJMV 2019augustine abellanaNo ratings yet