You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AUTOBIOGRAPHY and Genealogy of RizalDocument5 pagesAUTOBIOGRAPHY and Genealogy of RizalLuigi De Real80% (5)
- Sex, Gender and Health BiotechnologyDocument9 pagesSex, Gender and Health BiotechnologymoonchildNo ratings yet
- WWW - Srmuniv.ac - in Downloads Chapter-Ix Microbiological AssayDocument28 pagesWWW - Srmuniv.ac - in Downloads Chapter-Ix Microbiological AssayAlexiel NguyenNo ratings yet
- Certified Nursing AssistantDocument7 pagesCertified Nursing AssistantRina Ariestiana KandauNo ratings yet
- Autism Spectrum Disorders: A GuideDocument12 pagesAutism Spectrum Disorders: A Guidejudyblock100% (1)
- Implant Rehabilitation in The Edentulous Jaw: The "All-On-4" Immediate Function ConceptDocument8 pagesImplant Rehabilitation in The Edentulous Jaw: The "All-On-4" Immediate Function ConceptAnonymous i7fNNiRqh2No ratings yet
- Government of Nepal Ministry of Health and Population National Ayurveda Research and Training Center, Kirtipur, KathmanduDocument50 pagesGovernment of Nepal Ministry of Health and Population National Ayurveda Research and Training Center, Kirtipur, KathmanduAmit JoshiNo ratings yet
- Concept Map LungDocument1 pageConcept Map LungThea Eya FayeNo ratings yet
- Disrupted in Schizophrenia 1: Building Brains and Memories: David J Porteous and J Kirsty MillarDocument7 pagesDisrupted in Schizophrenia 1: Building Brains and Memories: David J Porteous and J Kirsty Millarrocambolescas perthNo ratings yet
- A Review of Disrupted-in-Schizophrenia-1 (Disc1) : Neurodevelopment, Cognition, and Mental ConditionsDocument9 pagesA Review of Disrupted-in-Schizophrenia-1 (Disc1) : Neurodevelopment, Cognition, and Mental Conditionsrocambolescas perthNo ratings yet
- Pittenger 2007Document22 pagesPittenger 2007rocambolescas perthNo ratings yet
- Basch 2004Document15 pagesBasch 2004rocambolescas perthNo ratings yet
- Glycinergic Transmission: Glycine Transporter Glyt2 in Neuronal PathologiesDocument10 pagesGlycinergic Transmission: Glycine Transporter Glyt2 in Neuronal Pathologiesrocambolescas perthNo ratings yet
- Evidence For An Expansion-Based Temporal SHH Gradient in Specifying Vertebrate Digit IdentitiesDocument12 pagesEvidence For An Expansion-Based Temporal SHH Gradient in Specifying Vertebrate Digit Identitiesrocambolescas perthNo ratings yet
- API Boarding Pass: Ankara Esenboga - MunichDocument6 pagesAPI Boarding Pass: Ankara Esenboga - Munichrocambolescas perthNo ratings yet
- 2,2 - Thiodiethanol: A New Water Soluble Mounting Medium For High Resolution Optical MicrosDocument9 pages2,2 - Thiodiethanol: A New Water Soluble Mounting Medium For High Resolution Optical Microsrocambolescas perthNo ratings yet
- FullDocument8 pagesFullrocambolescas perthNo ratings yet
- Review Polarity Proteins in Axon Specification and SynaptogenesisDocument14 pagesReview Polarity Proteins in Axon Specification and Synaptogenesisrocambolescas perthNo ratings yet
- Synaptic Actin Dysregulation, A Convergent Mechanism of Mental Disorders?Document7 pagesSynaptic Actin Dysregulation, A Convergent Mechanism of Mental Disorders?rocambolescas perthNo ratings yet
- Review Miniaturization of Nervous Systems and NeuronsDocument7 pagesReview Miniaturization of Nervous Systems and Neuronsrocambolescas perthNo ratings yet
- Note On Burden and Standard of Proof in Refugee ClaimsDocument7 pagesNote On Burden and Standard of Proof in Refugee Claimsrocambolescas perthNo ratings yet
- Cellular Mechanisms of Cerebellar LTD: Hervé Daniel, Carole Levenes and Francis CrépelDocument7 pagesCellular Mechanisms of Cerebellar LTD: Hervé Daniel, Carole Levenes and Francis Crépelrocambolescas perthNo ratings yet
- Molecular Mechanisms of Neuronal Migration Disorders, Quo Vadis?Document12 pagesMolecular Mechanisms of Neuronal Migration Disorders, Quo Vadis?rocambolescas perthNo ratings yet
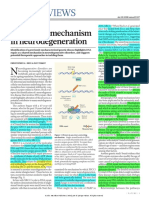
- News & Views: A Unifying Mechanism in NeurodegenerationDocument2 pagesNews & Views: A Unifying Mechanism in Neurodegenerationrocambolescas perthNo ratings yet
- PTEN: From Pathology To Biology: Maria Luisa Sulis and Ramon ParsonsDocument6 pagesPTEN: From Pathology To Biology: Maria Luisa Sulis and Ramon Parsonsrocambolescas perthNo ratings yet
- 1 s2.0 S0012160604004233 Main PDFDocument10 pages1 s2.0 S0012160604004233 Main PDFrocambolescas perthNo ratings yet
- Neural Circuits Underlying The Pathophysiology of Mood DisordersDocument11 pagesNeural Circuits Underlying The Pathophysiology of Mood Disordersrocambolescas perthNo ratings yet
- Review: Evolution of Vertebrates As Viewed From The CrestDocument9 pagesReview: Evolution of Vertebrates As Viewed From The Crestrocambolescas perthNo ratings yet
- Ptenless Means More: Bangyan Stiles, Matthias Groszer, Shunyou Wang, Jing Jiao, Hong WuDocument10 pagesPtenless Means More: Bangyan Stiles, Matthias Groszer, Shunyou Wang, Jing Jiao, Hong Wurocambolescas perthNo ratings yet
- 60Th Annual Refresher Course LecturesDocument59 pages60Th Annual Refresher Course Lecturesjands1930No ratings yet
- BMI FormulasDocument2 pagesBMI Formulasbarb201No ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- Phar LMRDocument5 pagesPhar LMRakshayNo ratings yet
- Management of ARDS in AdultsDocument2 pagesManagement of ARDS in AdultsCarlos PalominoNo ratings yet
- (General Scaffolding JRADocument7 pages(General Scaffolding JRA891629No ratings yet
- Effect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleDocument7 pagesEffect of COVID-19 On Doctor-Patient Relationship: Original Research ArticleMarlisa LionoNo ratings yet
- Methyldopa DYNAMED 2014Document19 pagesMethyldopa DYNAMED 2014Lalo AngelesNo ratings yet
- Insight Into NASH Pricing StrategiesDocument12 pagesInsight Into NASH Pricing Strategiesroni kalalaNo ratings yet
- Tampakan Brief ProfileDocument2 pagesTampakan Brief ProfilequeenroeviNo ratings yet
- Lesson 3: Implementing The Safety and Physical Activity PlanDocument12 pagesLesson 3: Implementing The Safety and Physical Activity PlanJopit Olavario RiveraNo ratings yet
- Dialog Bhs. Inggris DiareDocument4 pagesDialog Bhs. Inggris DiareJihan SalsabillaNo ratings yet
- Nle ReviewerdianemaydeeDocument809 pagesNle ReviewerdianemaydeeRaymark MoralesNo ratings yet
- Herniation Flash CardDocument4 pagesHerniation Flash CardAin GhazaliNo ratings yet
- Checklist MseDocument6 pagesChecklist MseHerlene Lyneth ZalamedaNo ratings yet
- Austin Pets Alive Cat Medication Chart 52F6Document6 pagesAustin Pets Alive Cat Medication Chart 52F6Shakira FerreiraNo ratings yet
- G 88 IDocument6 pagesG 88 IMayur MulyeNo ratings yet
- Culture: Dry Cough ToothacheDocument2 pagesCulture: Dry Cough ToothacheAgata KomendaNo ratings yet
- Tea BenefitsDocument13 pagesTea Benefitszhijie_ohNo ratings yet
- Antepartum Risk Factors For Postpartum Depression - A Follow Up Study Among Urban Women Living in Nairobi, KenyaDocument8 pagesAntepartum Risk Factors For Postpartum Depression - A Follow Up Study Among Urban Women Living in Nairobi, Kenyakartini ciatawiNo ratings yet
- Corneal Topography and TomographyDocument18 pagesCorneal Topography and TomographyPande GustianaNo ratings yet
- Modeling The Immunization of Healthcare SystemsDocument21 pagesModeling The Immunization of Healthcare SystemsTazkiyatun NufusNo ratings yet