You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- WATO EX-20,30,35 Service Manual - English - 20131025 PDFDocument258 pagesWATO EX-20,30,35 Service Manual - English - 20131025 PDFGustavo79% (29)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Urinary Tract Nursing Care GuideDocument38 pagesUrinary Tract Nursing Care GuideIke Agbor97% (33)
- Evamatic - Instructions For UseDocument24 pagesEvamatic - Instructions For UseCarl Azzopardi100% (2)
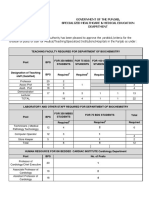
- Yardstick For Hospital PostsDocument124 pagesYardstick For Hospital Postsasghar_rana78100% (4)
- PBC Neck Contracture Anaesthesia TechniquesDocument17 pagesPBC Neck Contracture Anaesthesia TechniquescardiacanesthesiaNo ratings yet
- Regional Anesthesia and OutcomesDocument5 pagesRegional Anesthesia and OutcomespitriaNo ratings yet
- Clinical Science Questions and AnswersDocument30 pagesClinical Science Questions and Answersrakeeb qadriNo ratings yet
- Journal Club Presentation Postop HypoxemiaDocument37 pagesJournal Club Presentation Postop HypoxemiaNabin pokhrelNo ratings yet
- Informed Consent For Anesthesia CareDocument22 pagesInformed Consent For Anesthesia CareCatherine MorrisNo ratings yet
- Isoflurane, Sevoflurane and AnestesiDocument124 pagesIsoflurane, Sevoflurane and Anestesizidni fatayanNo ratings yet
- 10 1016@j Mpaic 2019 03 003 PDFDocument4 pages10 1016@j Mpaic 2019 03 003 PDFHerold23No ratings yet
- Veterinary Medicine Sci - 2022 - Saberfard - Effect of Medetomidine Midazolam Ketamine Propofol and Isoflurane OnDocument9 pagesVeterinary Medicine Sci - 2022 - Saberfard - Effect of Medetomidine Midazolam Ketamine Propofol and Isoflurane OnZanuba Ulya Haura cellinNo ratings yet
- Stanford Clinical Anesthesia TextbookDocument103 pagesStanford Clinical Anesthesia TextbookRishi Sharma100% (2)
- Ourse Yllabus Section I - College and University Catalog DataDocument5 pagesOurse Yllabus Section I - College and University Catalog DatabagusNo ratings yet
- 2309499017754106Document9 pages2309499017754106harumNo ratings yet
- GE Tec-7 Vaporizer - Maintenance ManualDocument48 pagesGE Tec-7 Vaporizer - Maintenance ManualLizzyNo ratings yet
- Anaesthetic Drug TablesDocument6 pagesAnaesthetic Drug TablesNanaNo ratings yet
- 664717ku PDFDocument19 pages664717ku PDFShankar Sex boyNo ratings yet
- Anesthesia Oral Board Review - Jessica A Lovich-SapolaDocument497 pagesAnesthesia Oral Board Review - Jessica A Lovich-Sapolazeispaul23No ratings yet
- Share the World's Leading Anesthesia MachineDocument6 pagesShare the World's Leading Anesthesia MachineSurta DevianaNo ratings yet
- Caudal anesthesia guideDocument27 pagesCaudal anesthesia guidepradeep daniel100% (1)
- F AnesthesiaDocument4 pagesF AnesthesiaArmandoGonzalezNo ratings yet
- Master Word ListshortDocument264 pagesMaster Word ListshortSoham ShaileshNo ratings yet
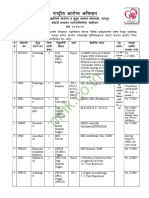
- NHM Nagpur Recruitment 2022Document5 pagesNHM Nagpur Recruitment 2022Bappasaheb PanditNo ratings yet
- NCP: Labor Stage 1 Active PhaseDocument10 pagesNCP: Labor Stage 1 Active PhaseJavie100% (3)
- Daftar PustakaDocument6 pagesDaftar PustakaAkhmad Ikhsan Prafita PutraNo ratings yet
- Clinical Management of Injured Birds-of-PreyDocument9 pagesClinical Management of Injured Birds-of-PreyLjón BjörnNo ratings yet
- Anesthesia NOTES PDFDocument22 pagesAnesthesia NOTES PDFdorquinloveNo ratings yet
- Stretch 2020Document7 pagesStretch 2020Caio OliveiraNo ratings yet
- Perioperative AnaphylaxisDocument23 pagesPerioperative AnaphylaxiscrackernetNo ratings yet