You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vital Signs Taking Quiz Answers & RationalesDocument2 pagesVital Signs Taking Quiz Answers & Rationalesroyale4eventzNo ratings yet
- Ischemic Heart DiseaseDocument55 pagesIschemic Heart DiseaseAndrassy Twinkle AlineaNo ratings yet
- Lisinopril Drug StudyDocument2 pagesLisinopril Drug StudyKristinelou Marie Reyna100% (1)
- Science 9 Quarter 1 (Week 1)Document7 pagesScience 9 Quarter 1 (Week 1)joyNo ratings yet
- Septimo, Ricka Marie D. - Labortaory No. 7. Frog Organ System Part 1Document4 pagesSeptimo, Ricka Marie D. - Labortaory No. 7. Frog Organ System Part 1Black RoseNo ratings yet
- Jaha 121 022505Document23 pagesJaha 121 022505Alexander FuksNo ratings yet
- Definition of ShockDocument29 pagesDefinition of Shockrazan asadNo ratings yet
- Instruction Manual Model EV4543 PDFDocument26 pagesInstruction Manual Model EV4543 PDFNathalia BaspeNo ratings yet
- Omron Blood Pressure Monitor M2 BasicDocument34 pagesOmron Blood Pressure Monitor M2 BasicEric Enrique Torres RojasNo ratings yet
- Reading The Holter ECG ReportDocument50 pagesReading The Holter ECG ReportGreta Tanushi KukaNo ratings yet
- Expository EssayDocument4 pagesExpository EssaytrevlynrobinsNo ratings yet
- Basic ECG InterpretationDocument62 pagesBasic ECG Interpretationmohannadalkwiese3No ratings yet
- Atypical Bypass Tracts 2019Document21 pagesAtypical Bypass Tracts 2019Võ Từ NhấtNo ratings yet
- Bio Homework Yr 12Document7 pagesBio Homework Yr 12tas xoNo ratings yet
- CPRDocument45 pagesCPRJames Elwood DoyolaNo ratings yet
- NT-proBNP Turbo - IMMULITE and IMMULITE 1000 - Rev 20 DXDCM 09017fe98029781e-1538195138152Document31 pagesNT-proBNP Turbo - IMMULITE and IMMULITE 1000 - Rev 20 DXDCM 09017fe98029781e-1538195138152LUIS DANIEL VAZQUEZ RAMIREZNo ratings yet
- Pearls of MRCP Part 2 PastestDocument111 pagesPearls of MRCP Part 2 PastestS TNo ratings yet
- RanolazineDocument20 pagesRanolazineashNo ratings yet
- Evaluation and Management of Premature Ventricular ComplexesDocument15 pagesEvaluation and Management of Premature Ventricular ComplexesJohnbray Castellanos DiazNo ratings yet
- Cathet Cardio Intervent - 2021 - Rocha Singh - Directional Atherectomy Before Paclitaxel Coated Balloon Angioplasty inDocument10 pagesCathet Cardio Intervent - 2021 - Rocha Singh - Directional Atherectomy Before Paclitaxel Coated Balloon Angioplasty inEnrique San NorbertoNo ratings yet
- Cir 0000000000000549Document120 pagesCir 0000000000000549MSNo ratings yet
- Junctional: TachycardiaDocument11 pagesJunctional: TachycardiachaiNo ratings yet
- Seminar - History Taking & Physical ExaminationDocument13 pagesSeminar - History Taking & Physical ExaminationsarxxxxNo ratings yet
- Nejmoa 1908655Document14 pagesNejmoa 1908655Pranvera ApostoliNo ratings yet
- Blood Consumption in Total Arterial Coronary Artery Bypass GraftingDocument16 pagesBlood Consumption in Total Arterial Coronary Artery Bypass Graftinginfo sekolahNo ratings yet
- Furosemide Side Effects - From FDA Reports - EHealthMeDocument3 pagesFurosemide Side Effects - From FDA Reports - EHealthMelaniNo ratings yet
- European J of Heart Fail - 2022 - Mullens - Renal Effects of Guideline Directed Medical Therapies in Heart Failure ADocument17 pagesEuropean J of Heart Fail - 2022 - Mullens - Renal Effects of Guideline Directed Medical Therapies in Heart Failure ALaura LizarazoNo ratings yet
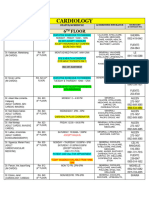
- CardiologyDocument2 pagesCardiologyLalin DaitolNo ratings yet
- NURS FPX 6011 Assessment 2 Evidence-Based Population Health Improvement PlanDocument5 pagesNURS FPX 6011 Assessment 2 Evidence-Based Population Health Improvement PlanEmma WatsonNo ratings yet
- Non Stress Test 1Document8 pagesNon Stress Test 1Ala'a Emerald AguamNo ratings yet