You might also like
- Statement of Purpose Example 45Document8 pagesStatement of Purpose Example 45akshayNo ratings yet
- Schneider Protection Application GuideDocument293 pagesSchneider Protection Application GuideFrancisco Martinez100% (1)
- 43 An Automated Deep Learning Based Software For Total Lung Volume Calculation and Lung 3D Model ReconstructionDocument8 pages43 An Automated Deep Learning Based Software For Total Lung Volume Calculation and Lung 3D Model ReconstructionHuy HoangNo ratings yet
- 3-D Segmentation AlgorithmDocument13 pages3-D Segmentation Algorithmkoushikraj900No ratings yet
- State-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant PlacementDocument7 pagesState-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant Placementanimeilove3No ratings yet
- BJR 71 846 9849380Document8 pagesBJR 71 846 9849380BitaNo ratings yet
- Prosch2012 (Jurnal 7)Document11 pagesProsch2012 (Jurnal 7)MayNo ratings yet
- Immobilisation FFFDocument8 pagesImmobilisation FFFSrinivas VenkataramanNo ratings yet
- Sarti 2012Document12 pagesSarti 2012mariaNo ratings yet
- Lee. C. D.Document14 pagesLee. C. D.GiovanniNo ratings yet
- Research Paper On Computed TomographyDocument8 pagesResearch Paper On Computed Tomographyafmcsmvbr100% (1)
- Icru Report 83Document103 pagesIcru Report 83Marlon SantosNo ratings yet
- 3D Printing Techniques in A Medical Setting: A Systematic Literature ReviewDocument21 pages3D Printing Techniques in A Medical Setting: A Systematic Literature ReviewIsabella GallardoNo ratings yet
- Research Article: Automated Quantification of Pneumothorax in CTDocument8 pagesResearch Article: Automated Quantification of Pneumothorax in CTAnnisa HidayatiNo ratings yet
- PravallikaDocument28 pagesPravallikaVegesana SumythriNo ratings yet
- An Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTDocument9 pagesAn Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTBounegta AhmedNo ratings yet
- PIIS093665552100368XDocument2 pagesPIIS093665552100368XAnharNo ratings yet
- 11.deep Learning Applications in Medical Image Analysis-Brain TumorDocument4 pages11.deep Learning Applications in Medical Image Analysis-Brain TumorVenky Naidu BalineniNo ratings yet
- Bio Med PaperDocument13 pagesBio Med PaperironmanjrpNo ratings yet
- LDNNET Towards Robust Classification of Lung Nodule and Cancer Using Lung Dense Neural NetworkDocument20 pagesLDNNET Towards Robust Classification of Lung Nodule and Cancer Using Lung Dense Neural Networkswathi sNo ratings yet
- J Ejmp 2020 02 017Document2 pagesJ Ejmp 2020 02 017Camilo SotomayorNo ratings yet
- Orp 3 CombDocument8 pagesOrp 3 CombControl de Equipos InternosNo ratings yet
- An Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of CancerDocument5 pagesAn Efficient Visualization and Segmentation of Lung CT Scan Images For Early Diagnosis of Cancermaruthi631No ratings yet
- Computer Methods and Programs in BiomedicineDocument12 pagesComputer Methods and Programs in BiomedicineJay PatelNo ratings yet
- EasyChair Preprint 545Document6 pagesEasyChair Preprint 545Greeni MarcoNo ratings yet
- CT Scan Research PapersDocument4 pagesCT Scan Research Paperspxihigrif100% (1)
- The Future of Hybrid Imaging-Part 2: PET/CT: Insights Into Imaging June 2011Document11 pagesThe Future of Hybrid Imaging-Part 2: PET/CT: Insights Into Imaging June 2011maaddy001No ratings yet
- Anapub Paper TemplateDocument10 pagesAnapub Paper Templatebdhiyanu87No ratings yet
- Eano GlioblastomaDocument10 pagesEano GlioblastomaMEILYN MEDINA FAÑANo ratings yet
- Robot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceDocument9 pagesRobot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceMamanya Fadhil HaniNo ratings yet
- Korir 2015Document11 pagesKorir 2015Rimo RimoNo ratings yet
- Radiation Dose Reduction Techniques For Chest CT Principles and Clinical ResultsDocument11 pagesRadiation Dose Reduction Techniques For Chest CT Principles and Clinical ResultsSantiago TapiaNo ratings yet
- Development and Research IssuesDocument3 pagesDevelopment and Research IssuesGAGANPREET SINGHNo ratings yet
- Technical Innovations & Patient Support in Radiation OncologyDocument9 pagesTechnical Innovations & Patient Support in Radiation OncologyDiana MitreaNo ratings yet
- Final DraftDocument18 pagesFinal Draftapi-334402872No ratings yet
- البحث الخامسDocument6 pagesالبحث الخامسAbd El-Rahman MohamedNo ratings yet
- GEC-ESTRO Recommendations III For HDR BTDocument8 pagesGEC-ESTRO Recommendations III For HDR BTClaudia Morales Ulloa100% (2)
- Prostate Segmentation ThesisDocument9 pagesProstate Segmentation Thesisgj9ggjry100% (2)
- Imaging in Polytrauma e Principles and Current ConceptsDocument8 pagesImaging in Polytrauma e Principles and Current ConceptsJJCONo ratings yet
- Lung Intervention by Using CT Fluoroscopy With Repository FrameworkDocument5 pagesLung Intervention by Using CT Fluoroscopy With Repository FrameworkerpublicationNo ratings yet
- Detection of Lung Nodules in Computed Tomography Images: F E U PDocument127 pagesDetection of Lung Nodules in Computed Tomography Images: F E U PcuongncNo ratings yet
- Bookshelf NBK592664Document13 pagesBookshelf NBK592664Ng Yi XuanNo ratings yet
- Different Styles of IGRTDocument10 pagesDifferent Styles of IGRTPeter CaldwellNo ratings yet
- Perfusion 1Document12 pagesPerfusion 1zixdiddyNo ratings yet
- CancerDocument9 pagesCancerMARIA JOSE RIVERA AVILANo ratings yet
- Pulmonary Airway Tissue Extraction For Lesion Detection Using HRCT ImagesDocument12 pagesPulmonary Airway Tissue Extraction For Lesion Detection Using HRCT ImagesArul SelviNo ratings yet
- Virtual SimulationDocument7 pagesVirtual SimulationNephtali LagaresNo ratings yet
- Utilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainDocument4 pagesUtilization Patterns of Multidetector Computed Tomography in Elective and Emergency Conditions: Indications, Exposure Risk, and Diagnostic GainJorge RodriguezNo ratings yet
- Screenshot 2024-05-10 at 2.21.25 AMDocument8 pagesScreenshot 2024-05-10 at 2.21.25 AMp6tsr5mg97No ratings yet
- Ghid Plex Brahial Conturaj PDFDocument7 pagesGhid Plex Brahial Conturaj PDFMiruna MafteiNo ratings yet
- Cine CT Withou A RespiratoryDocument20 pagesCine CT Withou A RespiratoryCan Trần KimNo ratings yet
- 2004 06578 PDFDocument19 pages2004 06578 PDFSumaNo ratings yet
- 2023-智能图像配准-attention guided refine and deformationDocument13 pages2023-智能图像配准-attention guided refine and deformationbo zhaoNo ratings yet
- Cone-Beam Computed Tomography and Its Applications in Dental and Maxillofacial RadiologyDocument11 pagesCone-Beam Computed Tomography and Its Applications in Dental and Maxillofacial RadiologyenzoNo ratings yet
- The Potential For Undertaking Slow CT Using A Modern CT ScannerDocument7 pagesThe Potential For Undertaking Slow CT Using A Modern CT ScannerAndreas RonaldNo ratings yet
- EHF2017 EK FinalPaperDocument9 pagesEHF2017 EK FinalPaperdanimalxNo ratings yet
- CT Scan in VeterinaryDocument4 pagesCT Scan in VeterinarySurajNo ratings yet
- Chapter 22 - Computed Tomography Simulation ProceduresDocument30 pagesChapter 22 - Computed Tomography Simulation ProceduresCarlo Gangcuangco ValdezNo ratings yet
- IEEE PAPER BATCH NO-03 A NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESDocument7 pagesIEEE PAPER BATCH NO-03 A NOVEL OBJECT DETECTION MODEL (YOLOv5) FOR IMPROVED LUNG NODULE IDENTIFICATION IN MEDICAL IMAGESS.GOPINATH5035No ratings yet
- Optimization in Radiology Eur J Med PhysDocument6 pagesOptimization in Radiology Eur J Med PhysobbebbiNo ratings yet
- Deepa Govind - Worker Health and Safety Awareness in 4 Steps Certificate 1Document1 pageDeepa Govind - Worker Health and Safety Awareness in 4 Steps Certificate 1api-354040213No ratings yet
- Assignment 1 - Article Summary WordDocument3 pagesAssignment 1 - Article Summary Wordapi-354040213No ratings yet
- Nejm 200005043421801Document8 pagesNejm 200005043421801api-354040213No ratings yet
- Health 1Document3 pagesHealth 1api-354040213No ratings yet
- EncoderDocument6 pagesEncoderHue BachNo ratings yet
- Compal Confidential: P1VE6 LA7071P Schematics DocumentDocument37 pagesCompal Confidential: P1VE6 LA7071P Schematics DocumentChristiam OrtegaNo ratings yet
- A231 - BKAM3023 Guidelines For Project 2-Service LearningDocument4 pagesA231 - BKAM3023 Guidelines For Project 2-Service LearningKhar FattNo ratings yet
- Street Photography - The Complete Guide (PDFDrive)Document130 pagesStreet Photography - The Complete Guide (PDFDrive)Paolo FasselliNo ratings yet
- Advanced Shipping Configuration With Websphere Commerce Calculation FrameworkDocument49 pagesAdvanced Shipping Configuration With Websphere Commerce Calculation FrameworkjaneeshpjNo ratings yet
- Wps SmawDocument1 pageWps SmawFedericoC67% (3)
- Ict National and Intl PoliciesDocument38 pagesIct National and Intl PoliciesWeendy Gayle T. VelilaNo ratings yet
- Montealegre-Training Proposal For Demonstration TeachingDocument12 pagesMontealegre-Training Proposal For Demonstration TeachingMarcela Consigo Ramos100% (1)
- Asr Install FlowDocument1 pageAsr Install FlowKamaldeep NainwalNo ratings yet
- Hareda 427466857Document86 pagesHareda 427466857Abhishek HandaNo ratings yet
- ZA550KL RF Hardware Trouble Shooting GuideDocument42 pagesZA550KL RF Hardware Trouble Shooting GuideWenderson FeltrinNo ratings yet
- Obtaining Wien's Displacement Law of Electromagnetic RadiationDocument10 pagesObtaining Wien's Displacement Law of Electromagnetic RadiationVikas TanwarNo ratings yet
- 03 SM-Series Hardware (SM150)Document81 pages03 SM-Series Hardware (SM150)John WickNo ratings yet
- C5-Mechanical Propertise of Hardened Concrete Base On Sample Made in C4Document8 pagesC5-Mechanical Propertise of Hardened Concrete Base On Sample Made in C4Muhammad khairinNo ratings yet
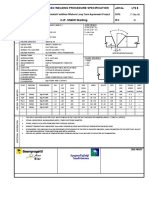
- TOTAL Welding Control Procedure Rev.2 PDFDocument116 pagesTOTAL Welding Control Procedure Rev.2 PDFWenney N Pali100% (1)
- 030 826 4Document2 pages030 826 4Diego Orlando Santos BuitragoNo ratings yet
- Igcse English A Past Paper Quesstions and AnswersDocument6 pagesIgcse English A Past Paper Quesstions and Answersmsml kml100% (2)
- Chapter 1 Managers and ManagementDocument32 pagesChapter 1 Managers and ManagementHaris FadillahNo ratings yet
- Atmel 8051 Microcontroller Family - Product Selection GuideDocument17 pagesAtmel 8051 Microcontroller Family - Product Selection GuideRahul GargNo ratings yet
- BCL IndustriesDocument1 pageBCL IndustriesRanjan BeheraNo ratings yet
- Recording Studio DesignDocument16 pagesRecording Studio DesignValentino FantiniNo ratings yet
- Marijauna Grow Basics - Jorge CervantesDocument242 pagesMarijauna Grow Basics - Jorge Cervantessosh_s97% (36)
- Pipelines and Pipe NetworksDocument56 pagesPipelines and Pipe NetworksAlok KumarNo ratings yet
- Credits: o 267 State Council For Technical Education Nagaland Semester Mark SheetDocument9 pagesCredits: o 267 State Council For Technical Education Nagaland Semester Mark SheetU Are NiceNo ratings yet
- Water Plane ComputationDocument14 pagesWater Plane ComputationAchonk Gio VelenoNo ratings yet
- Android Guide With Imtiaz Saifullah: Email: Ping/Text: +92-331-7370872Document6 pagesAndroid Guide With Imtiaz Saifullah: Email: Ping/Text: +92-331-7370872Ali Hassan NaqviNo ratings yet
- DS4600 Series For Retail: The Versatile Scanner That Does More For Your Retail OperationsDocument4 pagesDS4600 Series For Retail: The Versatile Scanner That Does More For Your Retail Operationsndfgdfs oishdfNo ratings yet
- Lab - #3. - Riverine HydraulicsDocument8 pagesLab - #3. - Riverine HydraulicsJuan CallesNo ratings yet