You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2006 - LIT102 - Philippine LiteratureDocument6 pages2006 - LIT102 - Philippine LiteratureKhail Vince ZoletaNo ratings yet
- Case Study For Ece Board ExamDocument82 pagesCase Study For Ece Board ExamSantos ArnelNo ratings yet
- Lidia Lentz - Final Project 1Document21 pagesLidia Lentz - Final Project 1api-528981875No ratings yet
- Electronics Engineers 04-2019 Room AssignmentDocument8 pagesElectronics Engineers 04-2019 Room AssignmentPRC BaguioNo ratings yet
- Tech Program EvaluationDocument5 pagesTech Program Evaluationapi-249448483No ratings yet
- GCSE Arabic 2017 Course PlannerDocument5 pagesGCSE Arabic 2017 Course PlannerlizaNo ratings yet
- Access 2 - Unit 1 - 1b (Repaired)Document3 pagesAccess 2 - Unit 1 - 1b (Repaired)Tâm Nguyễn ThanhNo ratings yet
- Lesson Plan: Teacher: Date: Time: School: ClassDocument2 pagesLesson Plan: Teacher: Date: Time: School: ClassDragana MilosevicNo ratings yet
- The ADDIE ModelDocument14 pagesThe ADDIE ModelPaul De Las Alas100% (1)
- Module 7 Assignment 7Document9 pagesModule 7 Assignment 7api-448231075No ratings yet
- A Reaction Paper About TaxDocument2 pagesA Reaction Paper About TaxsankNo ratings yet
- NAD Notice For Passed Out StudentsDocument1 pageNAD Notice For Passed Out StudentsLovneet SharmaNo ratings yet
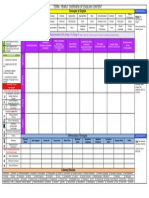
- English Planning Template-D Cherry-Cabramurrah PSDocument1 pageEnglish Planning Template-D Cherry-Cabramurrah PSS TANCRED100% (1)
- Jurnal International PDFDocument6 pagesJurnal International PDFFitriNo ratings yet
- MN7406 Assignment BriefDocument4 pagesMN7406 Assignment Briefnashra janNo ratings yet
- Chem3pracmanual 16-02-17Document346 pagesChem3pracmanual 16-02-17Naufal ShukriNo ratings yet
- T3903-390-02 SG-Ins Exc EN PDFDocument85 pagesT3903-390-02 SG-Ins Exc EN PDFgimNo ratings yet
- RUBRICS For Research Paper Defense, Peer, EtcDocument3 pagesRUBRICS For Research Paper Defense, Peer, EtcAnny YanongNo ratings yet
- Audit Log: Sheet . of Certification No - Name & InitialsDocument2 pagesAudit Log: Sheet . of Certification No - Name & InitialsmdksaeedNo ratings yet
- Rubrics For Musical PlayDocument2 pagesRubrics For Musical Playfaber vb80% (5)
- El Fili Chapter 11-20Document11 pagesEl Fili Chapter 11-20Satbir Singh50% (2)
- Summer Internship Sem5 Amity GuidelinesDocument13 pagesSummer Internship Sem5 Amity GuidelinesHughesNo ratings yet
- CV Leon Levstik ENG - PMDocument5 pagesCV Leon Levstik ENG - PMLeon LevstikNo ratings yet
- (Jupak) : Jurnal Pendidikan Agama KristenDocument26 pages(Jupak) : Jurnal Pendidikan Agama KristenJuwita ZendratoNo ratings yet
- Slide 1 Edu485 Bab 3Document30 pagesSlide 1 Edu485 Bab 3MUHAMMAD AZFAR AZIM MUHAMAD ARIFINNo ratings yet
- Alissa Nicole Levance: Raimondos, Ship Bottom, NJDocument2 pagesAlissa Nicole Levance: Raimondos, Ship Bottom, NJapi-487228391No ratings yet
- Class Record: IV Learners' Names Written Works Performance TasksDocument29 pagesClass Record: IV Learners' Names Written Works Performance TasksLance Aldrin AdionNo ratings yet
- Endorsement LetterDocument23 pagesEndorsement LetterGerry DuqueNo ratings yet
- CCEA GCSE Chemistry SpecificationDocument67 pagesCCEA GCSE Chemistry SpecificationastargroupNo ratings yet
- The Influence of Culture On AdvertisingDocument10 pagesThe Influence of Culture On AdvertisingZaniel Zayer HakariNo ratings yet