You might also like
- Sibo QuestionnaireDocument2 pagesSibo QuestionnaireNoorAk0% (1)
- History Taking Cheat SheetDocument1 pageHistory Taking Cheat SheetLaura ForsythNo ratings yet
- Pre Exam Surgical Notes 2Document166 pagesPre Exam Surgical Notes 2flor vickyNo ratings yet
- Gallstones in Pregnancy - UpToDateDocument51 pagesGallstones in Pregnancy - UpToDateLeira BarbosaNo ratings yet
- Enhanced Recovery After Colorectal Surgery - UpToDateDocument14 pagesEnhanced Recovery After Colorectal Surgery - UpToDateGeraldo FerreiraNo ratings yet
- Vascular Diseases (1 of 3)Document4 pagesVascular Diseases (1 of 3)Doctor GeneralNo ratings yet
- Schwartz Chapter 33 SpleenDocument20 pagesSchwartz Chapter 33 SpleenGay Solas Epalan100% (1)
- Hepatobiliary Notes 2.0Document18 pagesHepatobiliary Notes 2.0Sri VathanahNo ratings yet
- Acute Abdomen Causes Diagnosis TreatmentDocument8 pagesAcute Abdomen Causes Diagnosis Treatmentarum1992No ratings yet
- Acute AbdomenDocument5 pagesAcute AbdomenChris KingNo ratings yet
- Upper GIT BleedingDocument69 pagesUpper GIT BleedingSoleh Ramly100% (1)
- Acute Abdomen: - DefinitionDocument27 pagesAcute Abdomen: - DefinitionWorku KifleNo ratings yet
- Systemic Surgery NuggetsDocument17 pagesSystemic Surgery NuggetsAhmad UsmanNo ratings yet
- Matary GIT Surgery 2013 (WWW - Afriqa Sat - Com)Document328 pagesMatary GIT Surgery 2013 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAsuri KrishnaNo ratings yet
- 008 Plain X-Ray AbdomenDocument7 pages008 Plain X-Ray AbdomenAthul GurudasNo ratings yet
- Acute AbdomenDocument4 pagesAcute Abdomensarguss14No ratings yet
- Necrotizing FasciitisDocument7 pagesNecrotizing FasciitisjoycefrancielleNo ratings yet
- Benign Gynecologic LesionsDocument103 pagesBenign Gynecologic Lesions201286% (7)
- Approach To Thyroid NoduleDocument33 pagesApproach To Thyroid Nodulerajan kumar100% (5)
- PeritonitisDocument34 pagesPeritonitisabrar_zaidiNo ratings yet
- Aquifer Case 27Document4 pagesAquifer Case 27Dina KristevaNo ratings yet
- Damage Control SurgeryDocument31 pagesDamage Control SurgeryRose MendozaNo ratings yet
- Malignant Tumors of Uterus: DR Tahira RizwanDocument52 pagesMalignant Tumors of Uterus: DR Tahira RizwanSadia YousafNo ratings yet
- My Notes On SurgeryDocument22 pagesMy Notes On SurgeryRaffy GutmanNo ratings yet
- Diseases of The Esophagus DR Lapuz MCDDocument6 pagesDiseases of The Esophagus DR Lapuz MCDMiguel Cuevas Dolot100% (1)
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- AUBDocument26 pagesAUByayaslaras96No ratings yet
- Last Minute Revision Points LMRPDocument4 pagesLast Minute Revision Points LMRPbetsyNo ratings yet
- SurgeryDocument83 pagesSurgeryHamba Yg Betaubat100% (1)
- Case Study AllDocument22 pagesCase Study AllGeraldine Gallaron - CasipongNo ratings yet
- Pediatric Surgery Conditions of the Respiratory and Gastrointestinal SystemsDocument12 pagesPediatric Surgery Conditions of the Respiratory and Gastrointestinal SystemsRenatoCosmeGalvanJunior100% (1)
- Management of Acute Appendicitis in Adults - UpToDateDocument28 pagesManagement of Acute Appendicitis in Adults - UpToDateaulia rachman100% (1)
- Surgery CaseDocument43 pagesSurgery CaseAvni GuptaNo ratings yet
- Diagnosing & Treating CellulitisDocument18 pagesDiagnosing & Treating Cellulitismuthia saniNo ratings yet
- DDX - Gastrointestinal Disorders ChartDocument21 pagesDDX - Gastrointestinal Disorders Chartapi-26938624100% (2)
- Hypertensive Emergencies in The Emergency DepartmentDocument13 pagesHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNo ratings yet
- Mass in Epigastrium-2Document37 pagesMass in Epigastrium-2brown_chocolate87643100% (1)
- Peripheral Vascular Disease-1Document52 pagesPeripheral Vascular Disease-1Johiarra Madanglog Tabigne100% (1)
- Non-Variceal Upper GI Bleeding GuideDocument34 pagesNon-Variceal Upper GI Bleeding GuideChe Ainil ZainodinNo ratings yet
- Disorders of Sex Development (DSD) DevelopmentDocument40 pagesDisorders of Sex Development (DSD) DevelopmentAndi AdityaNo ratings yet
- Aquifer Case - Summary - FamilyMedicine21 - 12-YDocument10 pagesAquifer Case - Summary - FamilyMedicine21 - 12-YHyunsoo EllisNo ratings yet
- Acute AbdomenDocument19 pagesAcute AbdomenNazmi Z. MehmetiNo ratings yet
- Powerpoint: Disorders of The Thyroid GlandDocument67 pagesPowerpoint: Disorders of The Thyroid Glandj.doe.hex_87100% (1)
- HysterectomyDocument70 pagesHysterectomyYudhistira AdiNo ratings yet
- Venous DiseaseDocument45 pagesVenous DiseaseNinch Nagac100% (1)
- Hwee S O G A4 Spiral PDFDocument143 pagesHwee S O G A4 Spiral PDFeric sivaneshNo ratings yet
- Approach To Acute AbdomenDocument50 pagesApproach To Acute AbdomenAndie ArrNo ratings yet
- Scrotal SwellingDocument123 pagesScrotal SwellingLestari Amelia AdmNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Yamada's Handbook of GastroenterologyFrom EverandYamada's Handbook of GastroenterologyDr. Tadataka YamadaNo ratings yet
- A Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesFrom EverandA Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesJamalul Azizi Abdul RahamanNo ratings yet
- Immediate management of life-threatening abdominal problemsDocument3 pagesImmediate management of life-threatening abdominal problemsMike GNo ratings yet
- Effective Flexibility Training 90-Min-Toles2Document3 pagesEffective Flexibility Training 90-Min-Toles2Z SriNo ratings yet
- NCP BonoDocument2 pagesNCP BonomadypadNo ratings yet
- Australian Medical Council (Amc) Exam (Brief Overview)Document11 pagesAustralian Medical Council (Amc) Exam (Brief Overview)ahmerNo ratings yet
- Id MCQDocument6 pagesId MCQGalaleldin Ali100% (1)
- E070 PDFDocument37 pagesE070 PDFTroy FengNo ratings yet
- E070 PDFDocument37 pagesE070 PDFTroy FengNo ratings yet
- Infectious Disease PDFDocument13 pagesInfectious Disease PDFTroy FengNo ratings yet
- Infectious Disease PDFDocument13 pagesInfectious Disease PDFTroy FengNo ratings yet
- Neuroleptic Malignant Syndrome: Kathryn RosenblattDocument12 pagesNeuroleptic Malignant Syndrome: Kathryn RosenblattTroy FengNo ratings yet
- Neuroleptic Malignant Syndrome: Kathryn RosenblattDocument12 pagesNeuroleptic Malignant Syndrome: Kathryn RosenblattTroy FengNo ratings yet
- Rulebook Simpic2018Document17 pagesRulebook Simpic2018Troy FengNo ratings yet
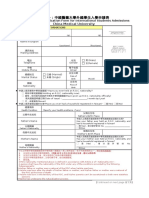
- China Medical University: Attachment 1: Application Form For International Students AdmissionsDocument3 pagesChina Medical University: Attachment 1: Application Form For International Students AdmissionsTroy FengNo ratings yet
- ELECTIVE TRAINING PROGRAMMEDocument4 pagesELECTIVE TRAINING PROGRAMMETroy FengNo ratings yet
- Ending Child Labor Abuse Through EducationDocument163 pagesEnding Child Labor Abuse Through EducationDuyBentley60% (5)
- AUF SOM - Dse of Small Intestine PDFDocument166 pagesAUF SOM - Dse of Small Intestine PDFYestin Reece Corpus ArcegaNo ratings yet
- A Gentle ReminderDocument1 pageA Gentle ReminderAlexiah mj BaradilloNo ratings yet
- Abdominal BloatingDocument1 pageAbdominal BloatingddmoorthiNo ratings yet
- HemorrhoidDocument12 pagesHemorrhoidAdelia Maharani DNo ratings yet
- Williamson CasestudyDocument31 pagesWilliamson Casestudyapi-369065120No ratings yet
- Epidemiology, Risk Factors and Treatment of Colorectal CarcinomaDocument19 pagesEpidemiology, Risk Factors and Treatment of Colorectal CarcinomaTaylorNo ratings yet
- Clinical Radiology For Surgical Conditions of The AbdomenDocument8 pagesClinical Radiology For Surgical Conditions of The AbdomenPreeti Joan Buxani100% (1)
- @ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverDocument10 pages@ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverHajjab AnasNo ratings yet
- Git GutDocument4 pagesGit GutAngelica Murillo Ang-AngcoNo ratings yet
- Kamus Icd - 10 Gigi Dan MulutDocument21 pagesKamus Icd - 10 Gigi Dan Mulutpoligigi kelapagadingNo ratings yet
- MOH Pocket Manual in General Surgery: Key Surgical Procedures and ConditionsDocument118 pagesMOH Pocket Manual in General Surgery: Key Surgical Procedures and ConditionsDrAlaa BawwatNo ratings yet
- Dental Plaque PresentationDocument10 pagesDental Plaque PresentationHesham100% (1)
- Daftar PustakaDocument2 pagesDaftar PustakaCitra Latika AgustiaNo ratings yet
- Presentation Liver CirrhosisDocument26 pagesPresentation Liver CirrhosisFaye Dominique Roxas PalmaresNo ratings yet
- Liver FibrosisDocument29 pagesLiver FibrosisAmira HelayelNo ratings yet
- Peptic Ulcer DiseaseDocument6 pagesPeptic Ulcer DiseaseNispap Harami RJNo ratings yet
- Clinical Approach to JaundiceDocument48 pagesClinical Approach to JaundiceSuranga Lakshitha PereraNo ratings yet
- Gastroenterology AscitesDocument2 pagesGastroenterology AscitesNour SamadNo ratings yet
- Chronic MegacolonDocument3 pagesChronic Megacolondrnareshkumar3281No ratings yet
- Drug Study DulcolaxDocument2 pagesDrug Study DulcolaxReisha Fungo0% (1)
- Non Invasive Imaging in NASHDocument3 pagesNon Invasive Imaging in NASHParul SoodNo ratings yet
- Book 1Document166 pagesBook 1Puput HepitasariNo ratings yet
- Presenting Complaint: ConstipationDocument5 pagesPresenting Complaint: ConstipationmiranaNo ratings yet
- Evaluation of The Adult With Abdominal Pain in The Emergency department-UpToDateDocument37 pagesEvaluation of The Adult With Abdominal Pain in The Emergency department-UpToDateAna Gabriela RodríguezNo ratings yet
- Jurnal Pengobatan GastritisDocument7 pagesJurnal Pengobatan Gastritisnana kuna100% (1)
- Ibs Isg-Inma Guidelines 2023Document25 pagesIbs Isg-Inma Guidelines 2023Nikhilesh YandamuriNo ratings yet
- ColonoscopyDocument5 pagesColonoscopyMa. Aira Jean PedroNo ratings yet
- PATHO 4-3 Diseases of The EsophagusDocument7 pagesPATHO 4-3 Diseases of The EsophagusMiguel Cuevas DolotNo ratings yet
- AJG article on diverticular disease and diverticulitisDocument7 pagesAJG article on diverticular disease and diverticulitisIrma Suriani DarwisNo ratings yet