You might also like
- Exercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509Document4 pagesExercise-Associated Numbness and Tingling in The Legs: For Editorial Comment See Page 1509herpthederpNo ratings yet
- 1812 FullDocument6 pages1812 FullWinston FontesNo ratings yet
- Causas de Isquemia Na MedulaDocument12 pagesCausas de Isquemia Na MeduladianaNo ratings yet
- 9.pediatric Dural Arteriovenous MalformationsDocument7 pages9.pediatric Dural Arteriovenous MalformationsNisa MahdiataraNo ratings yet
- 1 Abses SerebelumDocument6 pages1 Abses SerebelumseruniallisaaslimNo ratings yet
- EPIDURIALDocument3 pagesEPIDURIALALBERTO URIEL MONTAÑO CERVANTESNo ratings yet
- (10920684 - Neurosurgical Focus) Multiple Spinal Extradural Arachnoid Cysts Occurring in A ChildDocument4 pages(10920684 - Neurosurgical Focus) Multiple Spinal Extradural Arachnoid Cysts Occurring in A ChildRafael Mujica OreNo ratings yet
- Boroumand 2016Document3 pagesBoroumand 2016Winston FontesNo ratings yet
- A 7-Year-Old Boy Dying of Acute Encephalopathy: Case History Autopsy FindingsDocument4 pagesA 7-Year-Old Boy Dying of Acute Encephalopathy: Case History Autopsy FindingswillygopeNo ratings yet
- Descricion ofDocument5 pagesDescricion ofLlrss AdnNo ratings yet
- Carotid Cavernous FistulaDocument4 pagesCarotid Cavernous FistulaCarlos Del Carpio EnriquezNo ratings yet
- Brain 20 Ultrasonography 20 in 20 The 20 Premature 20 InfantDocument11 pagesBrain 20 Ultrasonography 20 in 20 The 20 Premature 20 InfantImin BuntaraNo ratings yet
- Spinal Cord EnhancementDocument3 pagesSpinal Cord EnhancementGabriel PinillaNo ratings yet
- Canine Choroid Plexus Tumor With Intracranial Dissemination Presenting As Multiple Cystic LesionsDocument5 pagesCanine Choroid Plexus Tumor With Intracranial Dissemination Presenting As Multiple Cystic LesionsMihai SavescuNo ratings yet
- Clinical Communications: Adults: Acute Lumbar Radiculopathy With Weak LegsDocument3 pagesClinical Communications: Adults: Acute Lumbar Radiculopathy With Weak LegsadeNo ratings yet
- Intracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyDocument2 pagesIntracranial Cavernomatous Hemangiomas As A Cause of Childhood Temporal Lobe EpilepsyPrateek Kumar PandaNo ratings yet
- A Rare Case of Vertebral Artery Pseudoaneurysmas An Iatrogenic ComplicationDocument4 pagesA Rare Case of Vertebral Artery Pseudoaneurysmas An Iatrogenic ComplicationIOSRjournalNo ratings yet
- (Radiology) RADIOLOGIDocument82 pages(Radiology) RADIOLOGIIrham KhairiNo ratings yet
- Combined Treatment of Surgery and Sclerotherapy For Sinus PericraniiDocument5 pagesCombined Treatment of Surgery and Sclerotherapy For Sinus Pericranii相壮壮No ratings yet
- Jurnal 1Document16 pagesJurnal 1Faisal Fitrah NasutionNo ratings yet
- 1882-Article Text-7722-1-10-20200608 PDFDocument6 pages1882-Article Text-7722-1-10-20200608 PDFRyanNo ratings yet
- The Management of Intracranial AbscessesDocument3 pagesThe Management of Intracranial AbscessesDio AlexanderNo ratings yet
- A Giant Spinal Arterial Aneurysm in A Child Presenting As Quadriparesis (Case Reports, Vol. 2013, Issue Aug20 1) (2013)Document4 pagesA Giant Spinal Arterial Aneurysm in A Child Presenting As Quadriparesis (Case Reports, Vol. 2013, Issue Aug20 1) (2013)negin.safari8227No ratings yet
- Dandy Walker MalformationDocument27 pagesDandy Walker MalformationNurul AtiqahNo ratings yet
- SD CobbDocument7 pagesSD CobbPam MoyolemaNo ratings yet
- Gejala Gangguan JiwaDocument8 pagesGejala Gangguan Jiwakevin stefanoNo ratings yet
- C+F-Syringomyelia and Hydro My Elia in Dogs and CatsDocument9 pagesC+F-Syringomyelia and Hydro My Elia in Dogs and Catstaner_soysurenNo ratings yet
- A Practical Approach To The Imaging Interpretation of Sphenoid Sinus PathologyDocument36 pagesA Practical Approach To The Imaging Interpretation of Sphenoid Sinus PathologyMario NarváezNo ratings yet
- Laryngeal TuberculosisDocument5 pagesLaryngeal TuberculosisastralmaniaNo ratings yet
- Diagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature ReviewDocument9 pagesDiagnostic Difficulties in Fibrous Dysplasia - A 5-Case Series and A Literature Reviewsolikin ikinNo ratings yet
- A Case of Deep Cerebral Venous Thrombosis Presenting Like Acute Necrotizing EncephalopathyDocument4 pagesA Case of Deep Cerebral Venous Thrombosis Presenting Like Acute Necrotizing EncephalopathySachin DangiNo ratings yet
- 4485 16580 2 PBDocument4 pages4485 16580 2 PBishu sNo ratings yet
- Intraosseous Arteriovenous Malformations Mimicking Malignant DiseaseDocument7 pagesIntraosseous Arteriovenous Malformations Mimicking Malignant DiseaseNm SNo ratings yet
- Spinal Epidural Abscess in Two CalvesDocument8 pagesSpinal Epidural Abscess in Two CalvesRachel AutranNo ratings yet
- Transcranial Ultrasound Doppler Parameters in CereDocument7 pagesTranscranial Ultrasound Doppler Parameters in CereImin BuntaraNo ratings yet
- NocardiaDocument6 pagesNocardiadocalsultanNo ratings yet
- Double-Outlet Left Ventricle and Vascular MalformationsDocument3 pagesDouble-Outlet Left Ventricle and Vascular MalformationsRaul UrietaNo ratings yet
- Atypical Kawasaki Disease Presenting As A RetrophaDocument3 pagesAtypical Kawasaki Disease Presenting As A RetrophaAlina TashnicNo ratings yet
- Vizcaino-Diaz2009 Rupture of Intracranial ArterialDocument7 pagesVizcaino-Diaz2009 Rupture of Intracranial ArterialModou NianeNo ratings yet
- Surgical Management of An Extensive Spinal EpiduraDocument5 pagesSurgical Management of An Extensive Spinal EpiduraqrscentralNo ratings yet
- Blunt Renal Trauma-Induced Hypertension in Pediatric Patients - A Single-Center ExperienceDocument9 pagesBlunt Renal Trauma-Induced Hypertension in Pediatric Patients - A Single-Center ExperienceChristian SihiteNo ratings yet
- Transcranial Ultrasound Doppler Parameters in Cerebral Vessels May Predict Intracerebral Hemorrhage in Preterm NewbornsDocument7 pagesTranscranial Ultrasound Doppler Parameters in Cerebral Vessels May Predict Intracerebral Hemorrhage in Preterm Newbornsrezza mochamadNo ratings yet
- 2019 - Chung Et Al-AnnotatedDocument6 pages2019 - Chung Et Al-AnnotatedCemal GürselNo ratings yet
- Large Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaDocument3 pagesLarge Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaJaya PrabhaNo ratings yet
- A Rare Case of Tubercular Pansinusitis With Orbital and Intracranial ExtensionDocument3 pagesA Rare Case of Tubercular Pansinusitis With Orbital and Intracranial Extensionnajmarani devi firdausNo ratings yet
- Convulsiones y HemianopsiaDocument2 pagesConvulsiones y HemianopsiadianisvillarrealNo ratings yet
- Absceso Cerebral en RN Asociado A Infeccion UmbilicalDocument5 pagesAbsceso Cerebral en RN Asociado A Infeccion UmbilicalAbrahamKatimeNo ratings yet
- A 6-Month-Old Infant Girl Presents With Neck Stiffness: SciencedirectDocument2 pagesA 6-Month-Old Infant Girl Presents With Neck Stiffness: Sciencedirectbuco ufmaNo ratings yet
- Blunt Neck Inj Slides 101217Document45 pagesBlunt Neck Inj Slides 101217taqadasabbasNo ratings yet
- Adem LikeDocument4 pagesAdem LikeRodrigo AriasNo ratings yet
- Neonatal Venous Cerebral Hemorrhage: Report of Two CasesDocument4 pagesNeonatal Venous Cerebral Hemorrhage: Report of Two Casesgrigorov_tNo ratings yet
- Case Report: Ruptured Spinal Arteriovenous Malformation: A Rare Cause of Paraplegia in PregnancyDocument5 pagesCase Report: Ruptured Spinal Arteriovenous Malformation: A Rare Cause of Paraplegia in Pregnancyilona ilincaNo ratings yet
- Ocular Histoplasmosis SyndromeDocument17 pagesOcular Histoplasmosis SyndromeDiana PSNo ratings yet
- Breathing Patterns in Children With Craniofacial Dysostosis and Hindbrain HerniationDocument7 pagesBreathing Patterns in Children With Craniofacial Dysostosis and Hindbrain HerniationDr.M.H. PatelNo ratings yet
- Retropharyngeal AbscessDocument3 pagesRetropharyngeal AbscessDwi Utari PratiwiNo ratings yet
- A Case Report of Hydrocephalus in A US Military RecruitDocument3 pagesA Case Report of Hydrocephalus in A US Military RecruitRomita PutriNo ratings yet
- Tuberculosis of The Spine: CT and MR Imaging FeaturesDocument6 pagesTuberculosis of The Spine: CT and MR Imaging FeaturesLuwiNo ratings yet
- Moya Sy 2 ChildrenDocument11 pagesMoya Sy 2 Childrenthomsoon01No ratings yet
- 264 2011 Article 1480Document6 pages264 2011 Article 1480Paul Mendez AguilarNo ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Ajr.13.11288 FixDocument12 pagesAjr.13.11288 FixmanalNo ratings yet
- A Novel Technique For The Treatment of Stages III.46 PDFDocument5 pagesA Novel Technique For The Treatment of Stages III.46 PDFmanalNo ratings yet
- Cold Burn Injuries in The UK: The 11-Year Experience of A Tertiary Burns CentreDocument8 pagesCold Burn Injuries in The UK: The 11-Year Experience of A Tertiary Burns CentremanalNo ratings yet
- Pengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahDocument7 pagesPengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahmanalNo ratings yet
- Congenital UrogenitalDocument6 pagesCongenital UrogenitalmanalNo ratings yet
- JCDR 8 DC22 - 2Document4 pagesJCDR 8 DC22 - 2manalNo ratings yet
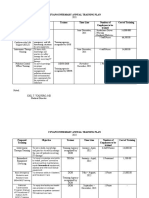
- Cuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingDocument3 pagesCuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingCuyapo Infirmary Lying-In HospitalNo ratings yet
- OASIS - 2 - 2020 - Risk of Obstetric Anal Sphincter Injuries (OASIS) and Anal Incontinence - A Meta-AnalysisDocument10 pagesOASIS - 2 - 2020 - Risk of Obstetric Anal Sphincter Injuries (OASIS) and Anal Incontinence - A Meta-AnalysisSamara MendesNo ratings yet
- Vocabulary (In and Around The Hospital)Document3 pagesVocabulary (In and Around The Hospital)Devi SetiawanNo ratings yet
- American Journal of RoentgenologyDocument9 pagesAmerican Journal of RoentgenologyPatricia GuzmanNo ratings yet
- Neonatology MCQDocument34 pagesNeonatology MCQNadeem Ur Rasool Sahibzada94% (31)
- Signs of LaborDocument40 pagesSigns of LaborDominicSavioNo ratings yet
- DSWD Act Ra 6972Document3 pagesDSWD Act Ra 6972Renel VelascoNo ratings yet
- Kode DiagnosaDocument6 pagesKode DiagnosaRoy SuhendraNo ratings yet
- Homeopathy Doctors Online ConsultationDocument16 pagesHomeopathy Doctors Online ConsultationKrishna PrasadNo ratings yet
- Chapter 18 Path and Lab Set BDocument4 pagesChapter 18 Path and Lab Set BBernard Paul Guinto0% (1)
- LasersDocument6 pagesLaserskomaill naqviNo ratings yet
- Bone RegenerationDocument360 pagesBone RegenerationMarc Balsells100% (1)
- Supplemental Exercise ManualDocument64 pagesSupplemental Exercise ManualAnikó Guttmann-Papp100% (1)
- Daftar Obat Lemari Nicu Picu Juni 2023Document2 pagesDaftar Obat Lemari Nicu Picu Juni 2023Bunga NurisnainiNo ratings yet
- A1c in PregnancyDocument20 pagesA1c in PregnancynandhinilpNo ratings yet
- Plica Mediana PeriduralDocument1 pagePlica Mediana PeriduralJorge PuertaNo ratings yet
- Actures of The Midfoot and ForefootDocument37 pagesActures of The Midfoot and ForefootMrHadezz LamerNo ratings yet
- Operative GynaecologyDocument59 pagesOperative GynaecologyArun Shree R0% (1)
- Week 2 - Motivation To Be A MidwifeDocument4 pagesWeek 2 - Motivation To Be A MidwifemitaNo ratings yet
- Uterine Artery in PreeclampsiaDocument27 pagesUterine Artery in PreeclampsiaedwincliffordNo ratings yet
- B OBGYN and UrologyDocument11 pagesB OBGYN and UrologyBryan BautistaNo ratings yet
- 985-Article Text-5131-1-10-20220801Document8 pages985-Article Text-5131-1-10-20220801armyta ddNo ratings yet
- Epidural AnesthesiaDocument7 pagesEpidural AnesthesiaAnn Michelle TarrobagoNo ratings yet
- Abnormal LaborDocument84 pagesAbnormal LaborMi MaymdNo ratings yet
- Aetna 1850 HD PlanDocument10 pagesAetna 1850 HD PlanNaveen ChintamaniNo ratings yet
- Annotated Bibliography 1Document4 pagesAnnotated Bibliography 1EloiseNo ratings yet
- Curriculum Vitae: ObjectiveDocument4 pagesCurriculum Vitae: ObjectiveMaheshSrikakulamNo ratings yet
- Republic Act No 10354Document16 pagesRepublic Act No 10354Ellen Glae DaquipilNo ratings yet
- Denture Conversion Manual 16.1 GBDocument28 pagesDenture Conversion Manual 16.1 GBRussu VadimNo ratings yet
- Universidad Iberoamericana: UnibeDocument3 pagesUniversidad Iberoamericana: UnibeMaria Paula Coss FernandezNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet