You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Blood BankingDocument9 pagesBlood BankingKimverlyn Balanay AgpaloNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Latin OrdinaryFormMassText PDFDocument25 pagesLatin OrdinaryFormMassText PDFAlbert ArominNo ratings yet
- Nosocomial: Infections in The Neonatal Intensive Care UnitDocument9 pagesNosocomial: Infections in The Neonatal Intensive Care UnitCleoanne Gallegos100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Parasitology Material Book (Medical.360°)Document320 pagesParasitology Material Book (Medical.360°)Muhammad Javed Gaba100% (1)
- Cells and Tissues Marieb 7Document92 pagesCells and Tissues Marieb 7Ryan Cadorna FontanillaNo ratings yet
- WEEK 9 Antimicrobial ChemotherapyDocument25 pagesWEEK 9 Antimicrobial Chemotherapyotaibynaif100% (2)
- Donning and DoffingDocument54 pagesDonning and Doffingsasa100% (1)
- Respiratory System Upper Respiratory DiseasesDocument32 pagesRespiratory System Upper Respiratory DiseasesPrince Rener Velasco Pera100% (1)
- AngeloDocument5 pagesAngeloRyan Cadorna Fontanilla100% (1)
- Research ExaminationDocument9 pagesResearch ExaminationRyan Cadorna FontanillaNo ratings yet
- 099 - Small Ruminant HealthDocument49 pages099 - Small Ruminant HealthSuraj_Subedi100% (1)
- Parasitology Revised SyllabusDocument6 pagesParasitology Revised Syllabusshlmr_foxNo ratings yet
- Teachers Evaluation ToolDocument2 pagesTeachers Evaluation ToolRyan Cadorna FontanillaNo ratings yet
- A Night and A Conversation Cerpen Bahasa InggrisDocument8 pagesA Night and A Conversation Cerpen Bahasa Inggrisnur hidayatullohNo ratings yet
- Effectiveness of Mother Tongue-Based InsDocument29 pagesEffectiveness of Mother Tongue-Based InsMhelBautistaPaderesNo ratings yet
- First Reading A Reading From The Acts of The ApostlesDocument2 pagesFirst Reading A Reading From The Acts of The ApostlesRyan Cadorna FontanillaNo ratings yet
- Prayers of The FaithfulDocument5 pagesPrayers of The FaithfulRyan Cadorna FontanillaNo ratings yet
- Mental Health Atlas - 2017 Questionnaire: Department of Mental Health and Substance Abuse World Health OrganizationDocument20 pagesMental Health Atlas - 2017 Questionnaire: Department of Mental Health and Substance Abuse World Health OrganizationMemmo AgirreNo ratings yet
- Be Not Afraid Arnel Aquino PDFDocument3 pagesBe Not Afraid Arnel Aquino PDFRyan Cadorna FontanillaNo ratings yet
- Sir Christian Local Related StudiesDocument1 pageSir Christian Local Related StudiesRyan Cadorna FontanillaNo ratings yet
- Supplemental Mental Health Questionnaire 508Document22 pagesSupplemental Mental Health Questionnaire 508JOY POMERNo ratings yet
- Bible VerseDocument1 pageBible VerseRyan Cadorna FontanillaNo ratings yet
- Enhancing LGU Capacities On DRR and CCDocument21 pagesEnhancing LGU Capacities On DRR and CCRyan Cadorna FontanillaNo ratings yet
- Republic of The Philippines Roxas Boulevard Corner San Luis Street Pasay CityDocument13 pagesRepublic of The Philippines Roxas Boulevard Corner San Luis Street Pasay CityRyan Cadorna FontanillaNo ratings yet
- Content ServerDocument23 pagesContent ServerRyan Cadorna FontanillaNo ratings yet
- Summer SceheduleDocument2 pagesSummer SceheduleRyan Cadorna FontanillaNo ratings yet
- 1Document9 pages1Ryan Cadorna FontanillaNo ratings yet
- Panel CommentsDocument1 pagePanel CommentsRyan Cadorna FontanillaNo ratings yet
- Answer KeyDocument92 pagesAnswer KeyRyan Cadorna FontanillaNo ratings yet
- Basic QuestionsDocument1 pageBasic QuestionsRyan Cadorna FontanillaNo ratings yet
- Tissues, Glands and Membranes: A. FunctionsDocument4 pagesTissues, Glands and Membranes: A. FunctionsRyan Cadorna FontanillaNo ratings yet
- Table of Conents FinalDocument3 pagesTable of Conents FinalRyan Cadorna FontanillaNo ratings yet
- Research Letter To The High School PrincipalDocument2 pagesResearch Letter To The High School PrincipalRyan Cadorna FontanillaNo ratings yet
- ChecklistDocument3 pagesChecklistRyan Cadorna FontanillaNo ratings yet
- June 18 SDocument4 pagesJune 18 SRyan Cadorna FontanillaNo ratings yet
- Table of Conents FinalDocument3 pagesTable of Conents FinalRyan Cadorna FontanillaNo ratings yet
- Master Animal Sciencesaster Animal SciencesDocument17 pagesMaster Animal Sciencesaster Animal SciencesRyan Cadorna FontanillaNo ratings yet
- A C K N o W L e D G e M e N TDocument1 pageA C K N o W L e D G e M e N TRyan Cadorna FontanillaNo ratings yet
- 5 Reasons Why You Should MDocument7 pages5 Reasons Why You Should MRyan Cadorna FontanillaNo ratings yet
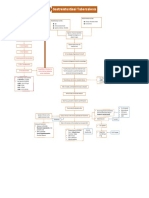
- Gastrointestinal Tuberculosis: PathogenesisDocument1 pageGastrointestinal Tuberculosis: Pathogenesis알파No ratings yet
- Kaya Kalp House Keeping StandardsDocument131 pagesKaya Kalp House Keeping StandardsAnuragMishraNo ratings yet
- Pediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OlderDocument3 pagesPediatric Tuberculosis: Specimen Collection For Analysis Sputum Specimens - Used in OldernadiahNo ratings yet
- Malaria Is A Mosquito-Borne Infectious Disease of Humans and OtherDocument3 pagesMalaria Is A Mosquito-Borne Infectious Disease of Humans and Otherkiran PoudelNo ratings yet
- Case Study With Teacher's Guide 2Document11 pagesCase Study With Teacher's Guide 2Mamati Chris MNo ratings yet
- Kurva WHODocument56 pagesKurva WHONatalia WaraNo ratings yet
- Post Graduate Academic Report Vion FinalDocument18 pagesPost Graduate Academic Report Vion FinalVishali RayapudiNo ratings yet
- Pneumonia in Children: IAP UG Teaching Slides 2015 16Document28 pagesPneumonia in Children: IAP UG Teaching Slides 2015 16Ananya Anaparthi100% (1)
- ReportDocument84 pagesReportNayyara ImtiazNo ratings yet
- Chapter 4 - Center For Food Safety and Applied NutritionDocument31 pagesChapter 4 - Center For Food Safety and Applied Nutritionsambath jayakumarNo ratings yet
- Annotated BibliographyDocument7 pagesAnnotated Bibliographyapi-202202577No ratings yet
- Medicine Matters - January 2018Document11 pagesMedicine Matters - January 2018Kim Kelley-WagnerNo ratings yet
- Research Paper (Apple Cider)Document2 pagesResearch Paper (Apple Cider)Trisha May Freires100% (3)
- 3 Biological Hazards PDFDocument9 pages3 Biological Hazards PDFdianNo ratings yet
- Polio OutbreakDocument3 pagesPolio OutbreakAyn Jel MayNo ratings yet
- ChickenpoxDocument5 pagesChickenpoxShan MunozNo ratings yet
- Diseases of Respiratory SystemDocument34 pagesDiseases of Respiratory SystemJerrald Meyer L. BayaniNo ratings yet
- Using Transition Words CorrectlyDocument4 pagesUsing Transition Words CorrectlyxhahaniNo ratings yet
- Rapid Molecular Testing TBDocument8 pagesRapid Molecular Testing TBNyonyo2ndlNo ratings yet
- Compre paraDocument103 pagesCompre paraDeniebev'z OrillosNo ratings yet
- Contact LensDocument6 pagesContact LensReno Prananditya AshafNo ratings yet