You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 5.case Presentation On Puerperial SepsisDocument38 pages5.case Presentation On Puerperial SepsisAngela Jolhnem Langhu92% (25)
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
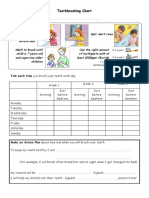
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
- Dental Anxiety Form 4 PDFDocument2 pagesDental Anxiety Form 4 PDFBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- Rubella On 22-2-2018Document48 pagesRubella On 22-2-2018farigNo ratings yet
- (D Doctor, P Patient) : Chapter 1: Molecular BiologyDocument13 pages(D Doctor, P Patient) : Chapter 1: Molecular BiologyVõ ĐứcNo ratings yet
- Rapidly Progressive Glomerulonephritis - P. Devarajan PDFDocument48 pagesRapidly Progressive Glomerulonephritis - P. Devarajan PDFHerman HermanNo ratings yet
- Miscellaneous ProtozoaDocument26 pagesMiscellaneous ProtozoaLycah Jyde PechuancoNo ratings yet
- Biozek MachE PDFDocument15 pagesBiozek MachE PDFTjmita RunieNo ratings yet
- VasDocument4 pagesVasadilNo ratings yet
- Inflammatory Disease of HeartDocument34 pagesInflammatory Disease of HeartLoma Waghmare (Jadhav)No ratings yet
- TREATMENTDocument9 pagesTREATMENTMae LibreNo ratings yet
- Captopril Drug StudyDocument7 pagesCaptopril Drug StudyKimzie Joy Basco100% (1)
- Right TKR SummaryDocument2 pagesRight TKR SummaryPrasad PotharajuNo ratings yet
- Threatened AbortionDocument1 pageThreatened AbortionTrisha SuazoNo ratings yet
- 2016 - Article - AbstractsForThe17thIPNACongres UrotomografiaDocument219 pages2016 - Article - AbstractsForThe17thIPNACongres UrotomografialeydyNo ratings yet
- © 2021 Lippincott Advisor - Treatments - HysterectomyDocument5 pages© 2021 Lippincott Advisor - Treatments - HysterectomyJoyJoy Tabada CalunsagNo ratings yet
- NCP Grading CriteriaDocument2 pagesNCP Grading CriteriaLecery Sophia WongNo ratings yet
- Clinical Practice Guidelines For The Management of Non-Specific Low Back Pain in Primary Care - An Updated OverviewDocument14 pagesClinical Practice Guidelines For The Management of Non-Specific Low Back Pain in Primary Care - An Updated OverviewCambriaChicoNo ratings yet
- Cyanosis Definition of Cyanosis in The MedicalDocument4 pagesCyanosis Definition of Cyanosis in The MedicalTavish B PrasadNo ratings yet
- GorantlaDocument18 pagesGorantlaapi-464986748No ratings yet
- Stomatology ReviewDocument17 pagesStomatology Reviewarya kumarNo ratings yet
- Seborrheic Dermatitis EmedicineDocument10 pagesSeborrheic Dermatitis EmedicineIkram IkramNo ratings yet
- VertigoDocument4 pagesVertigoshedNo ratings yet
- Perioperative NursingDocument15 pagesPerioperative Nursingmblanco.dchNo ratings yet
- Better Eyesight: WWW - Cleareyesight.infoDocument2 pagesBetter Eyesight: WWW - Cleareyesight.infoRay Richard SucaNo ratings yet
- WIDGB4 AK Utest Language 6Document4 pagesWIDGB4 AK Utest Language 6mintymouse881No ratings yet
- ShockDocument29 pagesShockKoRnflakes100% (4)
- Zoonoses 8Document404 pagesZoonoses 8Cagar Irwin Taufan0% (1)
- Acute Chronic PancreatitisDocument78 pagesAcute Chronic PancreatitisSirfaymons Sirfaymons Sirfaymons100% (2)
- Malaria: Dr. Harun Hudari, SPPDDocument49 pagesMalaria: Dr. Harun Hudari, SPPDEdvans HenryNo ratings yet
- Nephritic Syndrome - Armando HasudunganDocument14 pagesNephritic Syndrome - Armando HasudunganzahraaNo ratings yet
- Afar Biomarkers of Aging 2016 PDFDocument4 pagesAfar Biomarkers of Aging 2016 PDFPD SNo ratings yet