You might also like
- Treatment Approaches For Drug Addiction DrugfactsDocument10 pagesTreatment Approaches For Drug Addiction DrugfactsMustafa AlmasoudiNo ratings yet
- PISUAT AssignmentDocument9 pagesPISUAT AssignmentTan EXATNo ratings yet
- Hypnotic - WikipediaDocument16 pagesHypnotic - WikipediaHafsa AsifNo ratings yet
- Pharmacology of AddictionsDocument19 pagesPharmacology of AddictionsChaudhary Sumit TatranNo ratings yet
- Pharmacotherapy For Tobacco DependenceDocument19 pagesPharmacotherapy For Tobacco Dependencesinan sinanNo ratings yet
- Smoking CDocument10 pagesSmoking CDONALDNo ratings yet
- Smoking Cessation PresentationDocument24 pagesSmoking Cessation PresentationKhaulah Al-AzwarNo ratings yet
- Cannabinoid Replacement TherapyDocument4 pagesCannabinoid Replacement TherapyastrogliaNo ratings yet
- Alcoholism and Drug Dependence, Drug Delivery To TreatDocument7 pagesAlcoholism and Drug Dependence, Drug Delivery To TreatAndreea IorguNo ratings yet
- Beers List 350301Document22 pagesBeers List 350301Christine WaspNo ratings yet
- Antihypertensive in AkiDocument16 pagesAntihypertensive in AkiChia Yin NgNo ratings yet
- Review: Managing Smoking CessationDocument9 pagesReview: Managing Smoking CessationARAFAT MIAHNo ratings yet
- Drugs (Class 12) (Chemistry in Our Daily Life)Document40 pagesDrugs (Class 12) (Chemistry in Our Daily Life)Rohith MungathNo ratings yet
- Substance Abuse and Sleep DisorderDocument3 pagesSubstance Abuse and Sleep DisorderoladapoNo ratings yet
- Substance Related DisorderDocument35 pagesSubstance Related Disorderزينب عيسىNo ratings yet
- RECENT ADVANCES IN UNDERSTANDING AND MANAGEMENT OF CANNABIS, BENZODIAZEPINE AND TOBACCO DEPENDENCEDocument54 pagesRECENT ADVANCES IN UNDERSTANDING AND MANAGEMENT OF CANNABIS, BENZODIAZEPINE AND TOBACCO DEPENDENCEstpeter_agraNo ratings yet
- StimulantsDocument19 pagesStimulantsanagajose2003No ratings yet
- Gastrointestinal DrugsDocument49 pagesGastrointestinal DrugsMae Antonette OrlinaNo ratings yet
- Nicotine Dependence SyndromeDocument51 pagesNicotine Dependence SyndromeTesitaNo ratings yet
- Detox OpiateDocument50 pagesDetox OpiatePUSAT LATIHAN AADKNo ratings yet
- Beers List 350301Document22 pagesBeers List 350301Đình HưngNo ratings yet
- Monitoring Dan Evaluasi Penggunaan ObatDocument19 pagesMonitoring Dan Evaluasi Penggunaan ObatViona Prima DytaNo ratings yet
- Pallcare Pain Medsv6 - 17 8 2015Document5 pagesPallcare Pain Medsv6 - 17 8 20159mvsr5d9hhNo ratings yet
- Benzodiazepines Rational UseDocument25 pagesBenzodiazepines Rational UseMila PetrovicNo ratings yet
- Psychopharmacology in Psychopharmacology in Psychiatry PsychiatryDocument16 pagesPsychopharmacology in Psychopharmacology in Psychiatry PsychiatryHasnain HyderNo ratings yet
- 7 - ANS Affecting DrugsDocument92 pages7 - ANS Affecting DrugsShahpoor Ahmad ShirzadaNo ratings yet
- Managing Amphetamine Dependence: Malcolm BruceDocument8 pagesManaging Amphetamine Dependence: Malcolm BrucejuraiddinNo ratings yet
- Acep Equal Opiod Wave IiDocument43 pagesAcep Equal Opiod Wave IiJesse M. MassieNo ratings yet
- Detox OpiateDocument50 pagesDetox OpiatePUSAT LATIHAN AADKNo ratings yet
- Comprehensive Guide to Substance Abuse Diagnosis and TreatmentDocument3 pagesComprehensive Guide to Substance Abuse Diagnosis and TreatmentKuro HanabusaNo ratings yet
- Chapter 2 Pharmacotherapy For Smoking CessationDocument23 pagesChapter 2 Pharmacotherapy For Smoking CessationFoamm KitNo ratings yet
- Smoking Cessation AGU UpdatedDocument33 pagesSmoking Cessation AGU UpdatedRahaf AlhubailNo ratings yet
- Sedative Hypnotic DETOX For PHYSICIANS 2-11-14Document19 pagesSedative Hypnotic DETOX For PHYSICIANS 2-11-14Frank Raymond100% (1)
- 1.the Dentist s Quick Guide to Medical Conditions - 2015 - Weinberg - Appendix B Common Dental Drug InteractionsDocument11 pages1.the Dentist s Quick Guide to Medical Conditions - 2015 - Weinberg - Appendix B Common Dental Drug InteractionslindahamrunNo ratings yet
- Project ProposalDocument21 pagesProject Proposalfarhad khan100% (8)
- Tricyclic Antidepressants (Tcas) : Deprescribing Guide ForDocument4 pagesTricyclic Antidepressants (Tcas) : Deprescribing Guide ForEsteban Camilo Perez PerezNo ratings yet
- Mild Stimulants: Tobacco and Caffeine EffectsDocument38 pagesMild Stimulants: Tobacco and Caffeine EffectsOluwasegun OujemibolaNo ratings yet
- Naloxone in AdultsDocument8 pagesNaloxone in AdultsRoboschi StefaniaNo ratings yet
- Pharmacology Psychiatric MedicationsDocument36 pagesPharmacology Psychiatric Medicationsamasoud96 amasoud96No ratings yet
- Integrated Therapeutics IiiDocument14 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Anti Anxiety DrugsDocument15 pagesAnti Anxiety DrugsMr. Psycho SamNo ratings yet
- Bupropion Si NicotinaDocument17 pagesBupropion Si NicotinaRobert MovileanuNo ratings yet
- How To Encourage To Stop SmokingDocument12 pagesHow To Encourage To Stop SmokingSamNo ratings yet
- Understanding CNS DepressantsDocument49 pagesUnderstanding CNS DepressantsMirza Shaharyar BaigNo ratings yet
- 3 - Lec - PahrmaDocument45 pages3 - Lec - PahrmaDr Nimra MurtazaNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- NCM 106 NarcoticsDocument25 pagesNCM 106 NarcoticsMelchizedek Tagarino TorioNo ratings yet
- Cholinergic Drugs by MuneebDocument5 pagesCholinergic Drugs by MuneebMuneeb Ur RehmanNo ratings yet
- Depot Antipsychotic Medication Guidelines - PHA04 - February 2020 - 0Document29 pagesDepot Antipsychotic Medication Guidelines - PHA04 - February 2020 - 0Obinna AnozieNo ratings yet
- ABUSE OF TRANQUILIZER FixDocument6 pagesABUSE OF TRANQUILIZER Fixsusan bolengNo ratings yet
- Abuse of Tranquilizer (Diazepam)Document6 pagesAbuse of Tranquilizer (Diazepam)susan bolengNo ratings yet
- AnxiolyticsDocument8 pagesAnxiolyticsHengky_FandriNo ratings yet
- Designer DrugsDocument97 pagesDesigner DrugsAnonymous HackerNo ratings yet
- Unit 2Document12 pagesUnit 2parmarkeval1610No ratings yet
- Anxiolytics & Hypnotics Drugs Classification, Indications, and Side EffectsDocument21 pagesAnxiolytics & Hypnotics Drugs Classification, Indications, and Side EffectsabrihamNo ratings yet
- Addiction Management: Anas Elshafei & Shailee Trivedi Internal Medicine Core Rotation August 9, 2010 To October 29, 2010Document29 pagesAddiction Management: Anas Elshafei & Shailee Trivedi Internal Medicine Core Rotation August 9, 2010 To October 29, 2010sgolbariNo ratings yet
- Currentandexperimental Therapeuticsforthe TreatmentofopioidaddictionDocument12 pagesCurrentandexperimental Therapeuticsforthe Treatmentofopioidaddictionstein godoy pachecoNo ratings yet
- Treatment and SurgeryDocument7 pagesTreatment and Surgeryclem2xNo ratings yet
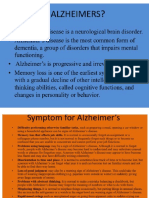
- AlzDocument20 pagesAlzDivyaNo ratings yet
- Spirituality vs Religiosity: What's the DifferenceDocument3 pagesSpirituality vs Religiosity: What's the DifferenceMae LibreNo ratings yet
- Sternberg's Triangular Theory of LoveDocument3 pagesSternberg's Triangular Theory of LoveMae LibreNo ratings yet
- 10 and 11Document6 pages10 and 11Mae LibreNo ratings yet
- Importance of Job Analysis in HRMDocument2 pagesImportance of Job Analysis in HRMMae LibreNo ratings yet
- An Inconvenient TruthDocument3 pagesAn Inconvenient TruthMae LibreNo ratings yet
- Journal Entry 4Document2 pagesJournal Entry 4Mae LibreNo ratings yet
- Journal 6Document5 pagesJournal 6Mae LibreNo ratings yet
- Journal 7Document4 pagesJournal 7Mae LibreNo ratings yet
- Journal 5Document3 pagesJournal 5Mae LibreNo ratings yet
- Journal Entry 2Document3 pagesJournal Entry 2Mae LibreNo ratings yet
- Zoo Frog Anatomy LabDocument6 pagesZoo Frog Anatomy LabMae LibreNo ratings yet
- Journal Entry 1Document3 pagesJournal Entry 1Mae LibreNo ratings yet
- Factors Prompting Students To Choose The Field of MedicineDocument23 pagesFactors Prompting Students To Choose The Field of MedicineMae LibreNo ratings yet
- Animal Form and Function in BiologyDocument3 pagesAnimal Form and Function in BiologyMae LibreNo ratings yet
- Little Albert ExperimentDocument3 pagesLittle Albert ExperimentMae LibreNo ratings yet
- Activity 1Document1 pageActivity 1Mae LibreNo ratings yet
- fpsyt-13-817927Document8 pagesfpsyt-13-817927Hemantajit GogoiNo ratings yet
- A Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalDocument66 pagesA Research Study On Attitude of Nurses Towards Relapse Prevention Among Psychiatric Patients in Federal Neuropsychiatric HospitalUsman Ahmad Tijjani100% (2)
- Alcoholism PINKAN PDFDocument68 pagesAlcoholism PINKAN PDFMartga Bella RahimiNo ratings yet
- Stages of Change ModelDocument4 pagesStages of Change Modelcarmen_georgescu1968No ratings yet
- JR Group ProposalDocument8 pagesJR Group Proposalapi-254132646100% (1)
- Bridgestone Behavioral Health Center: Cost-Volume-Profit (CVP) Analysis For Planning and ControlDocument8 pagesBridgestone Behavioral Health Center: Cost-Volume-Profit (CVP) Analysis For Planning and ControlAbbey Li0% (1)
- Hubungan Pengetahuan Tentang Hipertensi Dengan Perilaku Pencegahan Kekambuhan Hipertensi Pada Lansia Sarah Caroline, Arneliwati, Yulia Irvani DewiDocument8 pagesHubungan Pengetahuan Tentang Hipertensi Dengan Perilaku Pencegahan Kekambuhan Hipertensi Pada Lansia Sarah Caroline, Arneliwati, Yulia Irvani DewiRiie Napabii DuatigasembilandelapanNo ratings yet
- Competency PowerpointDocument24 pagesCompetency Powerpointapi-374116780No ratings yet
- Logic Models at Risk ProgrammingDocument24 pagesLogic Models at Risk ProgrammingNyree Austin Monroe100% (1)
- Alcohol Use DisorderDocument39 pagesAlcohol Use DisorderRibhav GuptaNo ratings yet
- Low Level Developmental Lead Exposure Does Not Predispose To Adul - 2020 - NeuroDocument14 pagesLow Level Developmental Lead Exposure Does Not Predispose To Adul - 2020 - NeuroClaudiaNo ratings yet
- Romantic Love - A Natural Addiction (Fisher Et Al, Frontiers in Psych, 2016)Document10 pagesRomantic Love - A Natural Addiction (Fisher Et Al, Frontiers in Psych, 2016)kimbeemanNo ratings yet
- Ebook BenzodiazepinesDocument26 pagesEbook BenzodiazepinesAnonymous Puj7S1tNo ratings yet
- Substance Use DisorderDocument20 pagesSubstance Use DisorderJana Marie CorpuzNo ratings yet
- In The Cave-Philosophy AddictionDocument2 pagesIn The Cave-Philosophy AddictionFAIFHAIHNo ratings yet
- Nine Points May-Jun 2010Document16 pagesNine Points May-Jun 2010TiburcincoNo ratings yet
- Adolescence ProblemDocument52 pagesAdolescence ProblememramyunusNo ratings yet
- Faith-Based Trauma-Informed Treatment For Sexual AddictionDocument24 pagesFaith-Based Trauma-Informed Treatment For Sexual AddictionTommy K. LiangNo ratings yet
- Therapeutic Community Ladderized Program (TCLPDocument19 pagesTherapeutic Community Ladderized Program (TCLPJais CampanillaNo ratings yet
- Relapse Prevention WorkbookDocument129 pagesRelapse Prevention WorkbookTania BeltranNo ratings yet
- Cognitive-Behavioral Treatment of Depression: A Three-Stage Model To Guide Treatment PlanningDocument9 pagesCognitive-Behavioral Treatment of Depression: A Three-Stage Model To Guide Treatment PlanningRija ChoudhryNo ratings yet
- Daily InventoryDocument3 pagesDaily InventoryYungston100% (2)
- Principles of Drug Addiction Treatment A Research Based Guide Third EditionDocument67 pagesPrinciples of Drug Addiction Treatment A Research Based Guide Third EditionКонстантин Крахмалев100% (1)
- Therapy WorksheetDocument47 pagesTherapy Worksheettyceiuk100% (2)
- Myths About AddictionDocument4 pagesMyths About AddictionCiedelle Honey Lou DimaligNo ratings yet
- Circuitos de La AdiccionDocument28 pagesCircuitos de La AdiccionJose Andres AlvarezNo ratings yet
- Nursing Care For Persons With Drug AddictionDocument25 pagesNursing Care For Persons With Drug AddictionMalik MashooqNo ratings yet
- Help Patients Understand Relapse As A Process and Event, and Learn How To Identify The Early Warning SignDocument3 pagesHelp Patients Understand Relapse As A Process and Event, and Learn How To Identify The Early Warning SignLurbieleeNo ratings yet
- Ebook PDF Nutrition Counseling and Education Skill Development 4th EditionDocument61 pagesEbook PDF Nutrition Counseling and Education Skill Development 4th Editionjefferson.kleckner559100% (50)
- Emotional DistressDocument12 pagesEmotional DistressfantasighNo ratings yet
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Drop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)From EverandDrop the Rock: Removing Character Defects: Steps Six and Seven (2nd. ed.)Rating: 4.5 out of 5 stars4.5/5 (52)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Food of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionFrom EverandFood of the Gods: The Search for the Original Tree of Knowledge: A Radical History of Plants, Drugs, and Human EvolutionRating: 4.5 out of 5 stars4.5/5 (117)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- The Language of Letting Go: Daily Meditations on CodependencyFrom EverandThe Language of Letting Go: Daily Meditations on CodependencyRating: 4.5 out of 5 stars4.5/5 (18)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)