You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The MAs Practice by CPAsDocument19 pagesThe MAs Practice by CPAsNikki Estores GonzalesNo ratings yet
- Mini Lesson 8 - UranusDocument2 pagesMini Lesson 8 - Uranuscaity_andrews17No ratings yet
- Clock Drawing Test: Nama Maba: Icha Nur Rohmah Nama Garda: PsychiatryDocument2 pagesClock Drawing Test: Nama Maba: Icha Nur Rohmah Nama Garda: PsychiatryRizky KaruniawatiNo ratings yet
- English Dialogue FixDocument7 pagesEnglish Dialogue FixRizky KaruniawatiNo ratings yet
- Perawat SelfieDocument18 pagesPerawat SelfieRizky KaruniawatiNo ratings yet
- BAB II Perawat SelfieDocument7 pagesBAB II Perawat SelfieRizky KaruniawatiNo ratings yet
- BAB II Perawat SelfieDocument7 pagesBAB II Perawat SelfieRizky KaruniawatiNo ratings yet
- Nilai Laboratorium Normal Pada Anak Dan DewasaDocument2 pagesNilai Laboratorium Normal Pada Anak Dan DewasaRizky KaruniawatiNo ratings yet
- NH1-16801110 PDFDocument8 pagesNH1-16801110 PDFRizky KaruniawatiNo ratings yet
- Psoriasis (10 Soal)Document64 pagesPsoriasis (10 Soal)Yuu Ayu'k Lifestar100% (1)
- Motivation Letter for LKMM 2 + SK FKUB TrainingDocument2 pagesMotivation Letter for LKMM 2 + SK FKUB TrainingRizky KaruniawatiNo ratings yet
- European Journal of Oncology Nursing: Emma Rowland, Gill Plumridge, Anna-Marie Considine, Alison MetcalfeDocument7 pagesEuropean Journal of Oncology Nursing: Emma Rowland, Gill Plumridge, Anna-Marie Considine, Alison MetcalfeRizky KaruniawatiNo ratings yet
- Spiritual Coping, Family History, and Perceived Risk For Breast Cancer-Can We Make Sense of It?Document13 pagesSpiritual Coping, Family History, and Perceived Risk For Breast Cancer-Can We Make Sense of It?Rizky KaruniawatiNo ratings yet
- Jurnal PrintDocument4 pagesJurnal PrintRizky KaruniawatiNo ratings yet
- Tugas EnglishDocument2 pagesTugas EnglishRizky KaruniawatiNo ratings yet
- European Journal of Oncology Nursing: Emma Rowland, Gill Plumridge, Anna-Marie Considine, Alison MetcalfeDocument7 pagesEuropean Journal of Oncology Nursing: Emma Rowland, Gill Plumridge, Anna-Marie Considine, Alison MetcalfeRizky KaruniawatiNo ratings yet
- Patient Education and CounselingDocument10 pagesPatient Education and CounselingRizky KaruniawatiNo ratings yet
- Genetika Psik2016Document56 pagesGenetika Psik2016Rizky KaruniawatiNo ratings yet
- Poems Questions N AnswersDocument18 pagesPoems Questions N AnswersAtiqahrafeeNo ratings yet
- PmqaDocument12 pagesPmqaAswathy AnilkumarNo ratings yet
- MRF ProjectDocument78 pagesMRF ProjectPrem Raj33% (3)
- ButohDocument27 pagesButohApoorva MahajanNo ratings yet
- Consumer Behavior Assignment: Stimulus GeneralizationDocument3 pagesConsumer Behavior Assignment: Stimulus GeneralizationSaurabh SumanNo ratings yet
- The Trickster MythDocument39 pagesThe Trickster MythLJ100% (1)
- Ghosts From The Perspective of Jyoti ADocument6 pagesGhosts From The Perspective of Jyoti Asurinder sangarNo ratings yet
- DedicationDocument8 pagesDedicationJohn Mathew BrionesNo ratings yet
- Programmed LearningDocument18 pagesProgrammed LearningRukhsana KhanNo ratings yet
- 1 Evolution of ManagementDocument56 pages1 Evolution of ManagementYASH SANJAY.INGLENo ratings yet
- District Reading Action PlanDocument4 pagesDistrict Reading Action PlanAnthony ChanNo ratings yet
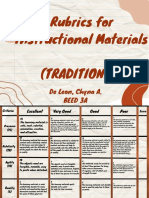
- (Rubrics) Traditional-Based Instructional MaterialDocument2 pages(Rubrics) Traditional-Based Instructional MaterialChyna De LeonNo ratings yet
- The Fellowship Service Manual of Co-Dependents AnonymousDocument39 pagesThe Fellowship Service Manual of Co-Dependents AnonymousJaime GutzmanNo ratings yet
- MCR003 A - B Assessment One 22T1Document2 pagesMCR003 A - B Assessment One 22T1Areej AhmedNo ratings yet
- Evaluating news reports rubricDocument1 pageEvaluating news reports rubricRhea M. VillartaNo ratings yet
- Scribd For Self-Improvement: A Roadmap To Personal GrowthDocument2 pagesScribd For Self-Improvement: A Roadmap To Personal GrowthABDESSALEM AGHRIBNo ratings yet
- Book Analysis on The Five People You Meet in HeavenDocument17 pagesBook Analysis on The Five People You Meet in HeavenMarifer Patricio100% (1)
- Gambler's FallacyDocument11 pagesGambler's Fallacyprashantsahu20078549No ratings yet
- 21st Century Skills Map: Designed in Cooperation With The Nation'S World Language Educ AtorsDocument21 pages21st Century Skills Map: Designed in Cooperation With The Nation'S World Language Educ Atorscasalim_34No ratings yet
- Daniela Severiano Iko2000540 Plac907 Dap Record 2023 - 4 CompressedDocument4 pagesDaniela Severiano Iko2000540 Plac907 Dap Record 2023 - 4 Compressedapi-682217085No ratings yet
- Presentations To Small GroupsDocument21 pagesPresentations To Small GroupsAashima GroverNo ratings yet
- Observation Sheet FormatDocument3 pagesObservation Sheet FormatNur Fatichatul LichaNo ratings yet
- Sams ResumeDocument3 pagesSams Resumeapi-355965919No ratings yet
- Ielts Task 2Document3 pagesIelts Task 2nilfiaNo ratings yet
- Molex Joining Forms - 26062018Document56 pagesMolex Joining Forms - 26062018tarunNo ratings yet
- How To Structure Quantitative Research QuestionsDocument12 pagesHow To Structure Quantitative Research QuestionsNICA ELLA TABUENANo ratings yet
- Verbal Advantage Powerful 3500 Vocabulary Words Yasser PDFDocument763 pagesVerbal Advantage Powerful 3500 Vocabulary Words Yasser PDFDharm D Veer Sorout67% (3)
- Unit Topic: Data Interpretation & Graphing Grade Level: 8 Stage 1 - Desired Results Content Standard/Established Goals(s)Document4 pagesUnit Topic: Data Interpretation & Graphing Grade Level: 8 Stage 1 - Desired Results Content Standard/Established Goals(s)VartyYeremianNo ratings yet