You might also like
- International Instruments on the Use of Antimicrobials across the Human, Animal and Plant SectorsFrom EverandInternational Instruments on the Use of Antimicrobials across the Human, Animal and Plant SectorsNo ratings yet
- White Paper How To Register Medicines AustraliaDocument23 pagesWhite Paper How To Register Medicines AustraliaShougandh GhoshNo ratings yet
- Who Expert Committee On Specifications For Pharmaceutical PreparationsDocument35 pagesWho Expert Committee On Specifications For Pharmaceutical PreparationsALVARONo ratings yet
- Regulatory Requirments of Tga & RowDocument29 pagesRegulatory Requirments of Tga & RowGautami UbhraniNo ratings yet
- Australian Public Assessment Report For Pertuzumab: Proprietary Product Name: Perjeta Sponsor: Roche Products Pty LTDDocument55 pagesAustralian Public Assessment Report For Pertuzumab: Proprietary Product Name: Perjeta Sponsor: Roche Products Pty LTDYunita TrianiNo ratings yet
- Auspar Omalizumab 210415Document32 pagesAuspar Omalizumab 210415maria-zinaida.dobreNo ratings yet
- WHO - Acute Diarrhea - Racecadotril - Utk Stop DiareDocument29 pagesWHO - Acute Diarrhea - Racecadotril - Utk Stop Diaremarkus_danusantosoNo ratings yet
- Australian Public Assessment Report For Sofosbuvir: Proprietary Product Name: Sovaldi Sponsor: Gilead Sciences Pty LTDDocument76 pagesAustralian Public Assessment Report For Sofosbuvir: Proprietary Product Name: Sovaldi Sponsor: Gilead Sciences Pty LTDCH NarimaneNo ratings yet
- TGADocument34 pagesTGAmisupatelNo ratings yet
- Public Summary: 1. Nature's Own Deep Sea Kelp 1000mg TabletDocument2 pagesPublic Summary: 1. Nature's Own Deep Sea Kelp 1000mg TabletRadoNo ratings yet
- Auspar Dimethyl Fumarate 131022Document87 pagesAuspar Dimethyl Fumarate 131022abhijit_gothoskar6039No ratings yet
- The Regulatory Standards For The Approval of Medical Devices in AustraliaDocument44 pagesThe Regulatory Standards For The Approval of Medical Devices in AustraliaRiesma TasomaraNo ratings yet
- DMF PDFDocument17 pagesDMF PDFAl RammohanNo ratings yet
- Srilaksmi 2017 Regulatory Requirements For Registration of API in US and EU PDFDocument17 pagesSrilaksmi 2017 Regulatory Requirements For Registration of API in US and EU PDFhira darNo ratings yet
- Review of Veterinary AntidotesDocument49 pagesReview of Veterinary AntidotesMarilena RaduNo ratings yet
- Labelling Drugs Poisons GuideDocument41 pagesLabelling Drugs Poisons GuideRashid AnzoomNo ratings yet
- CPG - Management of Drug Overdose and Poisoning May 2000Document453 pagesCPG - Management of Drug Overdose and Poisoning May 2000ririnNo ratings yet
- Therapeutic Good Administration: Australia (TGA)Document46 pagesTherapeutic Good Administration: Australia (TGA)sanjivNo ratings yet
- Evaluation of Certain Veterinary Drug Residues in FoodDocument111 pagesEvaluation of Certain Veterinary Drug Residues in Fooddan_redfield6258No ratings yet
- Kenya guidelines recall withdrawalsDocument18 pagesKenya guidelines recall withdrawalsSenthamaraiShanmughamNo ratings yet
- Triclosán_fs_PC-054901_1-Mar-10Document4 pagesTriclosán_fs_PC-054901_1-Mar-10Angel VegaNo ratings yet
- Consultation Proposed Clarification Certain Sports Supplements Are Therapeutic Goods - 0Document20 pagesConsultation Proposed Clarification Certain Sports Supplements Are Therapeutic Goods - 0lygiabuu28No ratings yet
- Who Emp qsm2008.3Document57 pagesWho Emp qsm2008.3VidyaNo ratings yet
- ACCC V Pfizer Kicks Off: Professional Pharmacy Services Now AvailableDocument3 pagesACCC V Pfizer Kicks Off: Professional Pharmacy Services Now AvailablepharmacydailyNo ratings yet
- Resource Technology CorporationDocument112 pagesResource Technology CorporationAnnurfa HikariNo ratings yet
- Regulatory Affairs PDFDocument27 pagesRegulatory Affairs PDFDipak BhingardeveNo ratings yet
- The Pharmaceutical Industry in AustraliaDocument59 pagesThe Pharmaceutical Industry in AustraliaHITESH MAKHIJANo ratings yet
- Retinoid Article 31 Referral Prac Assessment Report - enDocument29 pagesRetinoid Article 31 Referral Prac Assessment Report - enChindy MarselyaNo ratings yet
- EPA guidelines public health antimicrobial agentsDocument17 pagesEPA guidelines public health antimicrobial agentsdr. Febdi MaulanaNo ratings yet
- Consult Labelling Packaging Review 120524 Submission MaDocument8 pagesConsult Labelling Packaging Review 120524 Submission MamohammedNo ratings yet
- Thai FDA Drug Registration SystemDocument27 pagesThai FDA Drug Registration Systemelpaso25No ratings yet
- Organization of A PCR LaboratoryDocument16 pagesOrganization of A PCR LaboratoryNeagoeNo ratings yet
- Tga GuidelineDocument31 pagesTga GuidelineTushar Bambharoliya100% (2)
- Nonclinical safety evaluation pharmaceutical excipientsDocument12 pagesNonclinical safety evaluation pharmaceutical excipientsRich MacaryNo ratings yet
- FDA Guidelines For End-Product LAL Testing ValidationDocument13 pagesFDA Guidelines For End-Product LAL Testing Validationrajeev_s_nairNo ratings yet
- Craneetal 2019Document16 pagesCraneetal 2019บอส เลิศเกียรติรัชตะNo ratings yet
- Herbal Drug Regulation PDFDocument4 pagesHerbal Drug Regulation PDFPrathamesh KhotNo ratings yet
- Australian Guidelines For Drug RegistrationDocument30 pagesAustralian Guidelines For Drug Registrationswati_7381No ratings yet
- Pharmacy Laws and Regulations (Q:3%) : The Food and Drug AdministrationDocument7 pagesPharmacy Laws and Regulations (Q:3%) : The Food and Drug AdministrationHitomi Shiroshita100% (1)
- Drugs and Cosmetics Act and Schedule YDocument60 pagesDrugs and Cosmetics Act and Schedule YVaishali PatilNo ratings yet
- Poisons Standard 2011: Federal Register of Legislative Instruments F2011L01612Document369 pagesPoisons Standard 2011: Federal Register of Legislative Instruments F2011L01612Sara ChuangNo ratings yet
- Pharmacovigilance: A Protective Tool For Global Drug Safety AnalysisDocument8 pagesPharmacovigilance: A Protective Tool For Global Drug Safety AnalysisJeronim H'gharNo ratings yet
- Q3C (R8) FinalGuidance 2021-190TMOCC10.22.2021Document17 pagesQ3C (R8) FinalGuidance 2021-190TMOCC10.22.2021Keval PatelNo ratings yet
- Q3C(R8) Impurities: Guidance for Residual Solvents Updates PDEs for 3 SolventsDocument17 pagesQ3C(R8) Impurities: Guidance for Residual Solvents Updates PDEs for 3 SolventsMarco GarciaNo ratings yet
- 8416-Article Text-11800-1-10-20200127Document16 pages8416-Article Text-11800-1-10-20200127raginiNo ratings yet
- Pharmacy Daily For Mon 16 Jun 2014 - Methotrexate Deaths, Pharmacotherapy Sites Up, NZ Pharmacy of The Year, Call For COAG To Stay and Much MoreDocument3 pagesPharmacy Daily For Mon 16 Jun 2014 - Methotrexate Deaths, Pharmacotherapy Sites Up, NZ Pharmacy of The Year, Call For COAG To Stay and Much MorepharmacydailyNo ratings yet
- Regulatory Analysis On The Medical Use of Ephedrin - 2018 - Journal of Food andDocument6 pagesRegulatory Analysis On The Medical Use of Ephedrin - 2018 - Journal of Food andAisNo ratings yet
- V 2011 PR 01Document794 pagesV 2011 PR 01Jean Marie DjedjeNo ratings yet
- Regulatory Requirements For Approval of Over The Counter Drugs As Per Austrailian (Tga) GuidelinesDocument23 pagesRegulatory Requirements For Approval of Over The Counter Drugs As Per Austrailian (Tga) GuidelinesBaru Chandrasekhar RaoNo ratings yet
- EPA reregistration of streptomycin pesticideDocument5 pagesEPA reregistration of streptomycin pesticideMohamedNo ratings yet
- Chapter 2Document19 pagesChapter 2Rasha Samir Sryo100% (1)
- The Australian Clinical Trial HandbookDocument32 pagesThe Australian Clinical Trial HandbookAnvar KaleeckalNo ratings yet
- Who Di 33 1 MaintextDocument42 pagesWho Di 33 1 MaintextJose De La Cruz De La ONo ratings yet
- Clinical Study Design GuidelinesDocument23 pagesClinical Study Design Guidelinesrr48843No ratings yet
- Global Regulatory Strategy For Veterinary MedicinesDocument11 pagesGlobal Regulatory Strategy For Veterinary MedicinesCsar Sanchez Gracia50% (2)
- The Pharmaceutical Industry in Australia: Key Structural Characteristics and Supply ChainsDocument58 pagesThe Pharmaceutical Industry in Australia: Key Structural Characteristics and Supply ChainsVNcomerNo ratings yet
- 5991 1876enDocument32 pages5991 1876enBeatriz ReyesNo ratings yet
- 510 Pharmaceutical Industry: Drug Products, Labeling, and Packaging-PositionsDocument11 pages510 Pharmaceutical Industry: Drug Products, Labeling, and Packaging-PositionsAde Ayu Sukma bu acc plsNo ratings yet
- WHO Drug Informat Ion: Volume 36 Number 4 2022Document281 pagesWHO Drug Informat Ion: Volume 36 Number 4 2022anugrah rajaNo ratings yet
- Pharmacovigilance and Its Importance in Drug Regulation: An OverviewDocument16 pagesPharmacovigilance and Its Importance in Drug Regulation: An OverviewSarah ApriliaNo ratings yet
- This Is An Apple PDFDocument29 pagesThis Is An Apple PDFsanx19No ratings yet
- Xanax - FDADocument45 pagesXanax - FDAsanx19No ratings yet
- Oecd 425 PDFDocument27 pagesOecd 425 PDFHo Yoke MeiNo ratings yet
- Environment, Health & Safety NewsDocument25 pagesEnvironment, Health & Safety Newssanx19No ratings yet
- Marine PollutionDocument16 pagesMarine Pollutionsanx19No ratings yet
- Tables in National Plumbing CodeDocument4 pagesTables in National Plumbing CodeMartin GragasinNo ratings yet
- Textile Internship Report AlokDocument39 pagesTextile Internship Report AlokRahul TelangNo ratings yet
- HEAT EFFECTS (Cha 4) : Outline of Chapter OneDocument65 pagesHEAT EFFECTS (Cha 4) : Outline of Chapter OneAdam MekonnenNo ratings yet
- Managed Pressure Drilling MPD BrochureDocument5 pagesManaged Pressure Drilling MPD Brochureswaala4realNo ratings yet
- Thalassemia: Submitted By: Jovan Pierre C. Ouano Submitted To: Mark Gil T. DacutanDocument8 pagesThalassemia: Submitted By: Jovan Pierre C. Ouano Submitted To: Mark Gil T. DacutanJvnpierre AberricanNo ratings yet
- SteelsDocument72 pagesSteelsLLNo ratings yet
- With Machine Room - GAD-01Document1 pageWith Machine Room - GAD-01Nagarajan SNo ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- yudaturana,+Manajer+Jurnal,+dr +nelson+rev+2+ (162-172)Document12 pagesyudaturana,+Manajer+Jurnal,+dr +nelson+rev+2+ (162-172)Fath TiaraNo ratings yet
- HydrotherapyDocument7 pagesHydrotherapyGialys MoretaNo ratings yet
- Deskripsi (Caffein)Document4 pagesDeskripsi (Caffein)jibefahlaNo ratings yet
- Hook and Eye-Stories Form The MarginsDocument220 pagesHook and Eye-Stories Form The MarginsJefferson LiinNo ratings yet
- Sample Article Used by MeDocument14 pagesSample Article Used by MeMagnum OpusNo ratings yet
- Circuit Diagram:: Experiment No: 3 Title: Characteristics of Filament Lamp ObjectivesDocument2 pagesCircuit Diagram:: Experiment No: 3 Title: Characteristics of Filament Lamp ObjectivesAsrar Hussain BhatNo ratings yet
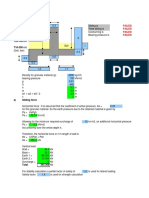
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- CD 0400 CH 4 X 100 ML: For in Vitro Diagnostic Use Only. LinearityDocument1 pageCD 0400 CH 4 X 100 ML: For in Vitro Diagnostic Use Only. LinearityNguyễn ThơiNo ratings yet
- STP1236 Eb.1415051 1 PDFDocument208 pagesSTP1236 Eb.1415051 1 PDFpaolaNo ratings yet
- vCloudPoint Sharing Computing Solution Data Sheet PDFDocument8 pagesvCloudPoint Sharing Computing Solution Data Sheet PDFkus satria dNo ratings yet
- Am 363 PDFDocument4 pagesAm 363 PDFsunsirNo ratings yet
- NOISE ANALYSISDocument16 pagesNOISE ANALYSISDiana Rose TapelNo ratings yet
- Petford & Atherton., 1996Document31 pagesPetford & Atherton., 1996Ivan Hagler Becerra VasquezNo ratings yet
- Effect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesDocument3 pagesEffect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesAbdifatah AhmedNo ratings yet
- Tables and Bar ChartsDocument7 pagesTables and Bar ChartsVictoria FedoseevaNo ratings yet
- Interpuls Novinki 2014Document64 pagesInterpuls Novinki 2014BaklanovaSVNo ratings yet
- PMR205 DR Shawn BakerDocument31 pagesPMR205 DR Shawn Bakerspiridon_andrei2011No ratings yet
- Textiles and Clothing SustaninabilityDocument134 pagesTextiles and Clothing Sustaninabilitydike100% (1)
- Violet Flame Clearing of The Heart ServiceDocument16 pagesViolet Flame Clearing of The Heart ServiceMySecret Gardenmdp82% (11)
- Guide to Quality Control Arrangements on SeedsDocument15 pagesGuide to Quality Control Arrangements on SeedsArun Kumar100% (1)
- Gem EscortingDocument7 pagesGem Escortingsuman sutharNo ratings yet