You might also like
- HB r762 Posesskode 2 05072018 81Document34 pagesHB r762 Posesskode 2 05072018 81marvinsahdNo ratings yet
- PSYCH 505 Case Study Core FunctionsDocument8 pagesPSYCH 505 Case Study Core FunctionsHugsNo ratings yet
- Iquanta Quant Formulae EbookDocument59 pagesIquanta Quant Formulae EbookonhaNo ratings yet
- DevwebdispDocument9 pagesDevwebdispJonathan Argel Maldonado JuarezNo ratings yet
- Birmingham Paper 3 PDFDocument587 pagesBirmingham Paper 3 PDFKashani DrShoaibNo ratings yet
- BrochureDocument2 pagesBrochureapi-375895852No ratings yet
- Spontanous Breakage - Nis PDFDocument22 pagesSpontanous Breakage - Nis PDFNaveen KarkiNo ratings yet
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 pagesBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura Cristina100% (1)
- Global Assessment of Functioning (GAF) Scale (DSM - IV Axis V)Document7 pagesGlobal Assessment of Functioning (GAF) Scale (DSM - IV Axis V)Lavinia AfloareiNo ratings yet
- Final Capstone PaperDocument15 pagesFinal Capstone Paperapi-478784238No ratings yet
- Humanistic Psychology, A New BreakthroughDocument5 pagesHumanistic Psychology, A New BreakthroughMarcelo Vial RoeheNo ratings yet
- SimSensei OverviewDocument1 pageSimSensei OverviewDom DeSiciliaNo ratings yet
- Delusional Disorder - An OverviewDocument12 pagesDelusional Disorder - An Overviewdrrlarry100% (1)
- Intervenciones Psicologicas Eficaces paraDocument18 pagesIntervenciones Psicologicas Eficaces paraLucía De Gregorio GarcíaNo ratings yet
- HAI (Short Version)Document4 pagesHAI (Short Version)Adeel AizadNo ratings yet
- SST Emergency-Medical Consent Form (SPANISH RMM)Document2 pagesSST Emergency-Medical Consent Form (SPANISH RMM)flonoelNo ratings yet
- Psychotropic-Induced Hyponatremia: A ReviewDocument9 pagesPsychotropic-Induced Hyponatremia: A ReviewJAVED ATHER SIDDIQUINo ratings yet
- Joshua Dodot Case StudyDocument2 pagesJoshua Dodot Case StudyJoshua Ringor100% (1)
- (Hollon, 2010) - The Cognitive RevolutionDocument12 pages(Hollon, 2010) - The Cognitive RevolutionEileen GarcíaNo ratings yet
- Screening For Personality Disorders Among PDFDocument14 pagesScreening For Personality Disorders Among PDFDrMartens AGNo ratings yet
- Psych Case StudyDocument13 pagesPsych Case Studyapi-662201129No ratings yet
- Calgary Depression Scale For Schizophrenia (CDSS)Document1 pageCalgary Depression Scale For Schizophrenia (CDSS)Edward Arthur IskandarNo ratings yet
- Pathological Narcissism and Narcissistic Personality DisorderDocument26 pagesPathological Narcissism and Narcissistic Personality DisorderAlex RodriguesNo ratings yet
- Clinical Interviews 2 Chap 4 Part 2Document47 pagesClinical Interviews 2 Chap 4 Part 2Ahmad Farooq100% (1)
- General Principles of The InterviewDocument76 pagesGeneral Principles of The InterviewEdi DrimaNo ratings yet
- Dowden Health Media: For Personal Use OnlyDocument8 pagesDowden Health Media: For Personal Use OnlyfernandoNo ratings yet
- Chapter 1. Introduction To PsychiatryDocument11 pagesChapter 1. Introduction To PsychiatryDiego Francesco Macali100% (1)
- PsychiatryDocument23 pagesPsychiatryNaveenKumarNo ratings yet
- Psych OutlineDocument4 pagesPsych OutlineSam Raven AndresNo ratings yet
- Gangguan BipolarDocument9 pagesGangguan BipolarNaomiNo ratings yet
- Schizophrenia & Other Psychotic DisordersabpsychDocument12 pagesSchizophrenia & Other Psychotic DisordersabpsychMary HiboNo ratings yet
- Coexistence of Folie Communique e and Folie SimultaneeDocument4 pagesCoexistence of Folie Communique e and Folie SimultaneeAna Rosa González Barroso0% (1)
- Eating Disorders: by Dr. Min Min Phyo 20 August 2019Document74 pagesEating Disorders: by Dr. Min Min Phyo 20 August 2019thu thuNo ratings yet
- Case - History PsychiatryDocument28 pagesCase - History PsychiatryMahmood SalahNo ratings yet
- Strasburger Et Al-2015-PsyCh JournalDocument8 pagesStrasburger Et Al-2015-PsyCh JournalPedro CardosoNo ratings yet
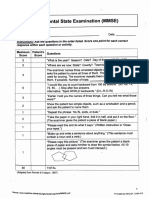
- Mini-Mental State Examination (MMSE)Document3 pagesMini-Mental State Examination (MMSE)Prescilla San PedroNo ratings yet
- Comparison Bet ICD & DSM PDFDocument18 pagesComparison Bet ICD & DSM PDFTiffany SyNo ratings yet
- Use of Psychotropics in PregnancyDocument24 pagesUse of Psychotropics in Pregnancymanahil waqas100% (1)
- Narcissistic Personality DisorderDocument12 pagesNarcissistic Personality DisorderYashika Jain -63No ratings yet
- Social Psychology-1Document23 pagesSocial Psychology-1Zubair Mahmood KamalNo ratings yet
- Substance Abuse: Steps For Handling The ProblemDocument8 pagesSubstance Abuse: Steps For Handling The ProblemRichNo ratings yet
- Understanding Motivation and Behavior ChangeDocument31 pagesUnderstanding Motivation and Behavior ChangeglaizaNo ratings yet
- Ybocs PDF Yale BrownDocument23 pagesYbocs PDF Yale BrowndevNo ratings yet
- Case Study Jared Tacey Youngstown State UniversityDocument13 pagesCase Study Jared Tacey Youngstown State Universityapi-402076669100% (1)
- Anxiety Dis. OCD and OtherDocument6 pagesAnxiety Dis. OCD and OtherIsabel CastilloNo ratings yet
- NSW Department of Health 2004 Suicide Risk Assessment and Management Protocols General Community Health ServiceDocument20 pagesNSW Department of Health 2004 Suicide Risk Assessment and Management Protocols General Community Health ServiceLuna MArinaNo ratings yet
- YBOCSDocument22 pagesYBOCSJanet FernandezNo ratings yet
- Catatonia PDFDocument9 pagesCatatonia PDFDanilo RibeiroNo ratings yet
- The Mental Illness SpectrumDocument4 pagesThe Mental Illness Spectrumfrancesca_valdivia100% (1)
- Case StudyDocument10 pagesCase StudyARABELLA FUNDARNo ratings yet
- Clinician Tabel Skizofrenia DSM VDocument4 pagesClinician Tabel Skizofrenia DSM VrayendrarenoNo ratings yet
- Psych Report of RDA by Ernie GarciaDocument3 pagesPsych Report of RDA by Ernie GarciaLe Ar NieNo ratings yet
- Detection of Bipolar Disorder BJP 2011 Young 3 4Document3 pagesDetection of Bipolar Disorder BJP 2011 Young 3 4Gede GiriNo ratings yet
- Suicide SeminarDocument47 pagesSuicide SeminarinikanikosNo ratings yet
- Protocolo AnsiedadDocument6 pagesProtocolo AnsiedadGabriela Espinosa ArreagaNo ratings yet
- A Case Study of A Mental DisorderDocument7 pagesA Case Study of A Mental DisorderMaurine TuitoekNo ratings yet
- Garb2005clinical Judgment and Decision MakingDocument25 pagesGarb2005clinical Judgment and Decision MakingNicolas Di Persia100% (1)
- The Code of Conduct For PsychologistsDocument3 pagesThe Code of Conduct For PsychologistsAnkit HasijaNo ratings yet
- Cultural Issue Schizophrenia IndiaDocument58 pagesCultural Issue Schizophrenia IndiaSam InvincibleNo ratings yet
- Week 2 (OSCE CASC Book II 2018-19) 03.09.2018Document48 pagesWeek 2 (OSCE CASC Book II 2018-19) 03.09.2018Andrew WdsmithNo ratings yet
- A Comparison Between The Mini Mental State Examination and The MoCA Test in SchizophreniaDocument6 pagesA Comparison Between The Mini Mental State Examination and The MoCA Test in SchizophreniaGuille NajarroNo ratings yet
- Without Stigma: About the Stigma and the Identity of the Mental IllnessFrom EverandWithout Stigma: About the Stigma and the Identity of the Mental IllnessNo ratings yet
- Spitzer Et Al., 2001Document8 pagesSpitzer Et Al., 2001Tania MartinezNo ratings yet
- The PHQ-9: Validity of A Brief Depression Severity MeasureDocument8 pagesThe PHQ-9: Validity of A Brief Depression Severity MeasuredokterkobuNo ratings yet
- The Direct Stiffness Method IDocument7 pagesThe Direct Stiffness Method Imiry89No ratings yet
- Table 1.15. Permissible Direct Tensile Stress: Grade of ConcreteDocument1 pageTable 1.15. Permissible Direct Tensile Stress: Grade of ConcretensiyamNo ratings yet
- Is 13039Document25 pagesIs 13039amitkdew70% (10)
- Determination of Concentration of Acetic Acid in VinegarDocument22 pagesDetermination of Concentration of Acetic Acid in VinegarFatin Izzati Hasnan100% (1)
- Unit 2 Problems FY21 Answers Thru 2.3Document11 pagesUnit 2 Problems FY21 Answers Thru 2.3Ankit UpadhyayNo ratings yet
- Venturi Effect: Jump To Navigationjump To SearchDocument5 pagesVenturi Effect: Jump To Navigationjump To SearchMonika KshNo ratings yet
- Nariyoshi Resume Aug2015Document1 pageNariyoshi Resume Aug2015api-295994597No ratings yet
- Numerical Analysis - Truncation and Taylor SeriesDocument25 pagesNumerical Analysis - Truncation and Taylor SeriesTommy FuNo ratings yet
- Cisco HyperFlex HX Data Platform Deploy Install v2 Demo GuideDocument40 pagesCisco HyperFlex HX Data Platform Deploy Install v2 Demo GuideAnonymous SR0AF3No ratings yet
- Acs Accounts 7b00153Document9 pagesAcs Accounts 7b00153ANUSREE T.CNo ratings yet
- Paper 4 Air Preheater Basket Cleaning PDFDocument43 pagesPaper 4 Air Preheater Basket Cleaning PDFMateus Pinheiro100% (2)
- Bahasa Inggris TeknikDocument5 pagesBahasa Inggris TeknikRakat NazZiNo ratings yet
- Chapter 2 Cast IronDocument9 pagesChapter 2 Cast IronHelen AdugnaNo ratings yet
- Geo p1Document4 pagesGeo p1VernonNo ratings yet
- Group IIIA: The Chemistry of AluminumDocument12 pagesGroup IIIA: The Chemistry of AluminumEvgeni GenevNo ratings yet
- Normatividad Colombiana Aplicada A La Seguridad y Salud en El TrabajoDocument273 pagesNormatividad Colombiana Aplicada A La Seguridad y Salud en El TrabajoJosé Aedo100% (1)
- TP3000WC ProWeatherStation User GuideDocument40 pagesTP3000WC ProWeatherStation User GuideRANDY SANTIAGONo ratings yet
- Defibrillators: What Is The Difference Between Monophasic and Biphasic Waveform Defibrillators?Document2 pagesDefibrillators: What Is The Difference Between Monophasic and Biphasic Waveform Defibrillators?Aurelia AlexandraNo ratings yet
- Quartiles Deciles and PercentilesDocument9 pagesQuartiles Deciles and PercentilesClerenda Mcgrady100% (1)
- NTSE SyllabusDocument5 pagesNTSE Syllabushardik guptaNo ratings yet
- Spe 372 Pa PDFDocument5 pagesSpe 372 Pa PDFМилица ДелићNo ratings yet
- Notes in Ring Theory: Paul Martin Dec 11, 2009 (Printed: May 8, 2012)Document36 pagesNotes in Ring Theory: Paul Martin Dec 11, 2009 (Printed: May 8, 2012)Mehrosh SeemabNo ratings yet
- Unit IDocument5 pagesUnit ISamyak MunotNo ratings yet
- Parametric Study of A Class of Arch Bridge ModelsDocument78 pagesParametric Study of A Class of Arch Bridge ModelsRamez Bou-RizkNo ratings yet
- Basic Electronics End Sem Paper PDFDocument4 pagesBasic Electronics End Sem Paper PDFSanket KumarNo ratings yet