You might also like
- Breast Disease: Diagnosis and Pathology, Volume 1From EverandBreast Disease: Diagnosis and Pathology, Volume 1Adnan AydinerNo ratings yet
- Management of Hereditary Colorectal Cancer: A Multidisciplinary ApproachFrom EverandManagement of Hereditary Colorectal Cancer: A Multidisciplinary ApproachJose G. GuillemNo ratings yet
- Borderline Tumor 1Document21 pagesBorderline Tumor 1Rovi WilmanNo ratings yet
- PJSS 66 3 Jul Sep 2011 3Document9 pagesPJSS 66 3 Jul Sep 2011 3Dwight AvelinoNo ratings yet
- Aab OvariumDocument3 pagesAab OvariumAgustinus FatollaNo ratings yet
- Endometrial HyperplasiaDocument12 pagesEndometrial HyperplasiaHenri KnafoNo ratings yet
- Prevalence and Asscociated Factors of Ovarian Cyst Malignancy: A Cros-Sectional Based Study in SurabayaDocument6 pagesPrevalence and Asscociated Factors of Ovarian Cyst Malignancy: A Cros-Sectional Based Study in SurabayakarenNo ratings yet
- JWH 2008 1068Document8 pagesJWH 2008 1068Khaled Loua-M'sNo ratings yet
- Green Journal ROMADocument9 pagesGreen Journal ROMAinvestorpatentNo ratings yet
- Bone Marrow Transplant For Metastatic Breast CancerDocument2 pagesBone Marrow Transplant For Metastatic Breast CancerGil LedermanNo ratings yet
- Breast Cancer During Pregnancy A Literature ReviewDocument7 pagesBreast Cancer During Pregnancy A Literature ReviewafmabreouxqmrcNo ratings yet
- Walsh 2005Document7 pagesWalsh 2005Catalin SavinNo ratings yet
- Detection of A Story CCM1 Frameshift Mutation in A Chinese Language Han Loved Ones Using Numerous Cerebral Cavernous MalformationsmqjvuDocument2 pagesDetection of A Story CCM1 Frameshift Mutation in A Chinese Language Han Loved Ones Using Numerous Cerebral Cavernous Malformationsmqjvumapmaple2No ratings yet
- Management of Ovarian Cysts: Review ArticleDocument10 pagesManagement of Ovarian Cysts: Review ArticleSania AzaliaNo ratings yet
- Journal BedahDocument15 pagesJournal BedahNovia NadhiraNo ratings yet
- Hippokratia 11 063Document4 pagesHippokratia 11 063Wiedya kristiantiNo ratings yet
- Fertility and Adjuvant Treatment in Young Women With Breast Cancer 2007 The BreastDocument7 pagesFertility and Adjuvant Treatment in Young Women With Breast Cancer 2007 The BreastRocky.84No ratings yet
- Jurnal Onko RiaDocument13 pagesJurnal Onko RiaMuzdatul KhairiahNo ratings yet
- Kapoor 2018Document8 pagesKapoor 2018angela_karenina_1No ratings yet
- Risk of Metachronous Ovarian Cancer After Cervical Cancer Ovarian ConservationDocument18 pagesRisk of Metachronous Ovarian Cancer After Cervical Cancer Ovarian ConservationJing WangNo ratings yet
- Accuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpDocument4 pagesAccuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpBmu CarreonNo ratings yet
- Goserelinversuscyclophosphamide, Methotrexate, and Fluorouracilasadjuvanttherapyinpremenopausalpatients Withnode-Positivebreastcancer:Thezoladexearlybreast CancerresearchassociationstudyDocument11 pagesGoserelinversuscyclophosphamide, Methotrexate, and Fluorouracilasadjuvanttherapyinpremenopausalpatients Withnode-Positivebreastcancer:Thezoladexearlybreast CancerresearchassociationstudyRaksha MoghariyaNo ratings yet
- Early Breast CancaerDocument17 pagesEarly Breast CancaerDwi Arnhilah Miranda100% (1)
- Current Status of Endometrial Carcinoma (Risk To Recurrence)Document6 pagesCurrent Status of Endometrial Carcinoma (Risk To Recurrence)Divika ShilvanaNo ratings yet
- 5926 21334 1 PBDocument3 pages5926 21334 1 PBM. K. AdilNo ratings yet
- Jonat 2002Document8 pagesJonat 2002KunalNo ratings yet
- Referensi 3Document13 pagesReferensi 3tofan widyaNo ratings yet
- Triple-Negative Breast Cancer CHEMO PDFDocument13 pagesTriple-Negative Breast Cancer CHEMO PDFVikash SinghNo ratings yet
- Adnexal Masses in Pregnancy: Surgery Compared With ObservationDocument6 pagesAdnexal Masses in Pregnancy: Surgery Compared With ObservationAgustinus FatollaNo ratings yet
- Pennant Et Al-2016-BJOG - An International Journal of Obstetrics & Gynaecology FichaDocument8 pagesPennant Et Al-2016-BJOG - An International Journal of Obstetrics & Gynaecology Fichaoctavio davilaNo ratings yet
- Modesitt 2003Document6 pagesModesitt 2003Evan QuirozNo ratings yet
- Peprah 2018Document7 pagesPeprah 2018Dewa OkaNo ratings yet
- Study of Management in Patient With Ectopic Pregnancy: Key WordsDocument3 pagesStudy of Management in Patient With Ectopic Pregnancy: Key WordsparkfishyNo ratings yet
- New Microsoft Office Word DocumentDocument11 pagesNew Microsoft Office Word DocumentMihaela AndreiNo ratings yet
- Pregnancy As A Risk Factor For Thyroid Cancer ProgressionDocument4 pagesPregnancy As A Risk Factor For Thyroid Cancer ProgressionErika AvilaNo ratings yet
- Introduction To Breast CancerDocument4 pagesIntroduction To Breast CancerEzzati AizaNo ratings yet
- Nejmoa 2207586Document15 pagesNejmoa 2207586Mirabela CretuNo ratings yet
- Meijers Heijboer2001Document6 pagesMeijers Heijboer2001Market PlusNo ratings yet
- Acta 90 405Document6 pagesActa 90 405Eftychia GkikaNo ratings yet
- GYNECOLOGY SYSTEM: CASE REPORT ON JUVENILE GRANULOSA CELL TUMORDocument4 pagesGYNECOLOGY SYSTEM: CASE REPORT ON JUVENILE GRANULOSA CELL TUMORCecepNo ratings yet
- Advances in Screening, Diagnosis, and Treatment ofDocument7 pagesAdvances in Screening, Diagnosis, and Treatment ofBastomy EkaNo ratings yet
- BPJ Vol 14 No 4 P 1993-2005Document13 pagesBPJ Vol 14 No 4 P 1993-2005Dr. Shraddha YadavNo ratings yet
- Cervical Cancer in Pregnancy Review LiteratureDocument5 pagesCervical Cancer in Pregnancy Review Literaturef1gisofykyt3100% (1)
- Borderline Ovarian Cancer: Understanding Tumors of Low Malignant PotentialDocument8 pagesBorderline Ovarian Cancer: Understanding Tumors of Low Malignant Potentialamarendra WardhanaNo ratings yet
- 1 s2.0 S0039128X1300086X MainDocument4 pages1 s2.0 S0039128X1300086X MainA NNo ratings yet
- Progestogen TreatmentDocument6 pagesProgestogen TreatmentIndah HaneNo ratings yet
- Nejme2032499 PDFDocument2 pagesNejme2032499 PDFBladimir CentenoNo ratings yet
- 17 Iajps17102017 PDFDocument3 pages17 Iajps17102017 PDFBaru Chandrasekhar RaoNo ratings yet
- 410-Article Text-1440-1-10-20211018Document7 pages410-Article Text-1440-1-10-20211018silviatengkerNo ratings yet
- Management of Paget Disease of The Breast With RadiotherapyDocument8 pagesManagement of Paget Disease of The Breast With RadiotherapyAndreas RonaldNo ratings yet
- Kanker Payudara Akibat ReceptorDocument7 pagesKanker Payudara Akibat ReceptorMuhammad Aditya firdausNo ratings yet
- Manchester Experience 2021Document10 pagesManchester Experience 2021Sara HossamNo ratings yet
- Scand J Work Environ Health:3-7: Environmental Risk Factors of Breast CancerDocument6 pagesScand J Work Environ Health:3-7: Environmental Risk Factors of Breast CancerKhush BhullarNo ratings yet
- Green Top Guidelines 12Document15 pagesGreen Top Guidelines 12Arafath AkramNo ratings yet
- Prognostic Value of p53 Gene in Ovarian Cancer: - Maj Obstet 172 Rauf Dan Masadah Ginekol IndonesDocument5 pagesPrognostic Value of p53 Gene in Ovarian Cancer: - Maj Obstet 172 Rauf Dan Masadah Ginekol IndonesDini MedyaniNo ratings yet
- Cervical Cancer in The Pregnant PopulationDocument15 pagesCervical Cancer in The Pregnant PopulationLohayne ReisNo ratings yet
- Infertility and Preg Post CADocument18 pagesInfertility and Preg Post CAMariajanNo ratings yet
- Ung Thư VúDocument16 pagesUng Thư VúVăn LêNo ratings yet
- Updates in Cervical Cytology: 90 Years of ProgressDocument11 pagesUpdates in Cervical Cytology: 90 Years of Progressmohamaed abbasNo ratings yet
- 2011 Article 342Document4 pages2011 Article 342Gilang IrwansyahNo ratings yet
- Scan Doc with CamScanner AppDocument1 pageScan Doc with CamScanner Apprashid793No ratings yet
- LIST OF REGISTERED PROPERTY DEALERS IN BAHAWALPURDocument11 pagesLIST OF REGISTERED PROPERTY DEALERS IN BAHAWALPURrashid793No ratings yet
- Job OpeningsDocument3 pagesJob Openingsrashid793No ratings yet
- T2140 - Webinars 28 Sep 2020 - JOINING INSTRUCTIONSDocument1 pageT2140 - Webinars 28 Sep 2020 - JOINING INSTRUCTIONSrashid793No ratings yet
- Application Form For Residential Plots 15-08-2020Document2 pagesApplication Form For Residential Plots 15-08-2020rashid793No ratings yet
- Salary Lahore High CourtDocument1 pageSalary Lahore High Courtrashid793No ratings yet
- Daily Gantry Crane Inspection ChecklistDocument1 pageDaily Gantry Crane Inspection Checklistrashid793No ratings yet
- 40-F030-120E Driver PreShift Inspection-Daily RevADocument1 page40-F030-120E Driver PreShift Inspection-Daily RevArashid793No ratings yet
- Group Life Insurance For Policybazaar Motor Comprehensive Policy CustomersDocument4 pagesGroup Life Insurance For Policybazaar Motor Comprehensive Policy Customersrashid793No ratings yet
- 40-F030-120E Driver PreShift Inspection-Daily RevADocument1 page40-F030-120E Driver PreShift Inspection-Daily RevArashid793No ratings yet
- 40-F030-120E Driver PreShift Inspection-Daily RevADocument1 page40-F030-120E Driver PreShift Inspection-Daily RevArashid793No ratings yet
- Al Bidiya Supermarket Midweek OfferDocument3 pagesAl Bidiya Supermarket Midweek Offerrashid793No ratings yet
- Mod5 PDFDocument14 pagesMod5 PDFdeepak pandeyNo ratings yet
- Crawler Crane Daily Inspection ChecklistDocument1 pageCrawler Crane Daily Inspection Checklistrashid7930% (1)
- Construction Safety Supervisor Experience LetterDocument2 pagesConstruction Safety Supervisor Experience LetterMohamed Ibrahim AhamedRasmi89% (9)
- M3L1 LNDocument7 pagesM3L1 LNswapna44No ratings yet
- FormulaDocument8 pagesFormularashid793No ratings yet
- Construction Safety Supervisor Experience LetterDocument2 pagesConstruction Safety Supervisor Experience LetterMohamed Ibrahim AhamedRasmi89% (9)
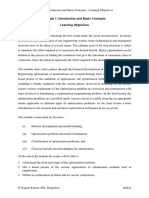
- M1L3 LNDocument7 pagesM1L3 LNnagesha_basappa865No ratings yet
- M1 Learning ObjectivesDocument2 pagesM1 Learning ObjectivesnnernNo ratings yet
- Quick Revision Sheet H&S LawDocument2 pagesQuick Revision Sheet H&S Lawrashid793No ratings yet
- 5 M Application Form PDFDocument2 pages5 M Application Form PDFikramishereNo ratings yet
- Plumbing NotesDocument53 pagesPlumbing NotesArvee VillamorNo ratings yet
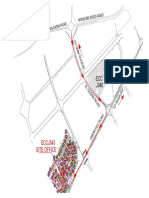
- J343 - Location Map PDFDocument1 pageJ343 - Location Map PDFrashid793100% (1)
- Candidate Data Sheet: All Fields Are MandatoryDocument1 pageCandidate Data Sheet: All Fields Are Mandatoryrashid793No ratings yet
- Payment of Wages Act, 1936 - DocDocument10 pagesPayment of Wages Act, 1936 - DocSaba KhanNo ratings yet
- Prestressing SteelDocument12 pagesPrestressing SteelBhuidhar VermaNo ratings yet
- 2 - Salary PackageDocument3 pages2 - Salary Packagerashid793No ratings yet
- ORKGet StartedDocument339 pagesORKGet Startedrashid793No ratings yet
- Q1 TLE 10-12 Wellness Massage NCII Module 4Document21 pagesQ1 TLE 10-12 Wellness Massage NCII Module 4Kim Caguioa100% (2)
- Quadas 2Document10 pagesQuadas 2Lya QillahNo ratings yet
- MSOSH Academy Training Calendar 2020Document23 pagesMSOSH Academy Training Calendar 2020Muhammad FizreeNo ratings yet
- Tips For Triage NursesDocument4 pagesTips For Triage NursesCamille05No ratings yet
- DepEd Puerto Princesa City School Bridging Gaps ReportDocument2 pagesDepEd Puerto Princesa City School Bridging Gaps ReportJazzele LongnoNo ratings yet
- Memo 19-0376 Absences - BacaneDocument2 pagesMemo 19-0376 Absences - BacaneEnrryson SebastianNo ratings yet
- 01 DI Industrial Product Division Catalogue 2022Document984 pages01 DI Industrial Product Division Catalogue 2022SatheeshNo ratings yet
- Iep Worksheet ActivitiesDocument7 pagesIep Worksheet Activitiesapi-346406650No ratings yet
- Golden RiceDocument6 pagesGolden RiceJoshua AgravioNo ratings yet
- Kair Profile DressCompanyDocument24 pagesKair Profile DressCompanySreenivas Chowdary VaddineniNo ratings yet
- Thoracentesis ProDocument6 pagesThoracentesis ProRaidis PangilinanNo ratings yet
- Treat Chronic DacryocystitisDocument34 pagesTreat Chronic DacryocystitisAriyanie NurtaniaNo ratings yet
- Stroke & Neurological Disease Conference: Ninth AnnualDocument2 pagesStroke & Neurological Disease Conference: Ninth Annualyos_peace86No ratings yet
- Agency ProjectDocument14 pagesAgency Projectapi-304517936No ratings yet
- ANE BelakangDocument3 pagesANE BelakangGustomo PanantroNo ratings yet
- UKFP 2024 Applicant HandbookDocument20 pagesUKFP 2024 Applicant HandbookS Abi GunnamNo ratings yet
- Assignment DNHEDocument9 pagesAssignment DNHEmohitNo ratings yet
- Nepal 3 Year Interim Plan EngDocument42 pagesNepal 3 Year Interim Plan Engparbatdhungana100% (1)
- Private Health Institutions LawDocument22 pagesPrivate Health Institutions LawShankar SanyalNo ratings yet
- Proper urine collection maximizes lab test diagnosisDocument26 pagesProper urine collection maximizes lab test diagnosisClaryse EroyNo ratings yet
- Dhama 2021Document18 pagesDhama 2021Share linkNo ratings yet
- Lifelong Learning of the Elderly in JapanDocument6 pagesLifelong Learning of the Elderly in JapanAzida AlzahariNo ratings yet
- Mental: Your Health MattersDocument2 pagesMental: Your Health MattersKrsnaPentayahNo ratings yet
- Module 7 Mental Health and Well-Being in Middle and Late AdolescenceDocument22 pagesModule 7 Mental Health and Well-Being in Middle and Late AdolescenceFaith CubillaNo ratings yet
- The Natural Way To A Healthy HealingDocument111 pagesThe Natural Way To A Healthy HealingAnjanaNo ratings yet
- Histology Report 10-06-2022Document2 pagesHistology Report 10-06-2022chloedee30No ratings yet
- 10.1007@s11065 020 09443 7Document14 pages10.1007@s11065 020 09443 7José NettoNo ratings yet
- Infographic The Body As A Source of Big Data HealthIT InfographicDocument1 pageInfographic The Body As A Source of Big Data HealthIT InfographiciHT²100% (1)
- Annemarie Mol Mind Your PlateDocument19 pagesAnnemarie Mol Mind Your PlateantonadiaborgesNo ratings yet
- Js 1 3rd Term Phe E-NotesDocument18 pagesJs 1 3rd Term Phe E-NotesGloria Ngeri Dan-Orawari50% (2)