You might also like
- Internal Medicine Progress Note TemplateDocument2 pagesInternal Medicine Progress Note Templatehector100% (1)
- 60 Affirmations For PeaceDocument21 pages60 Affirmations For PeacehectorNo ratings yet
- Ebook - Artes Marciais - DR Jwing-Ming Yang - Tai Chi - Qigong - The Secret of YouthDocument33 pagesEbook - Artes Marciais - DR Jwing-Ming Yang - Tai Chi - Qigong - The Secret of YouthsabaraceifadorNo ratings yet
- Mukharjee Regimen 321Document16 pagesMukharjee Regimen 321shreyahospital.motinagarNo ratings yet
- The AOA Guide:: How To Succeed in The Third-Year ClerkshipsDocument25 pagesThe AOA Guide:: How To Succeed in The Third-Year Clerkshipshector100% (1)
- SketchyIM Check List PDFDocument5 pagesSketchyIM Check List PDFhectorNo ratings yet
- 10class Biology Bits - (Em) RRDocument35 pages10class Biology Bits - (Em) RRsekkharchandra50% (2)
- Caa HemorrhageDocument7 pagesCaa HemorrhageGabriel Septiana CitraNo ratings yet
- First Aid For Common Unintentional InjuriesDocument13 pagesFirst Aid For Common Unintentional InjuriesORENJI ORENJI ORENJINo ratings yet
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- Concept MapDocument4 pagesConcept MapChelsyann FerolinoNo ratings yet
- Lees BurnDocument20 pagesLees BurnJennifer DixonNo ratings yet
- Circulatory System FrogDocument9 pagesCirculatory System FrogLeticiaNo ratings yet
- The Healing Power of WaterDocument22 pagesThe Healing Power of WaterMNo ratings yet
- The Last Bloodcarver by Vanessa LeDocument15 pagesThe Last Bloodcarver by Vanessa LeMacmillan KidsNo ratings yet
- Imaging Findings of Vascular Lesions in The Head and NeckDocument7 pagesImaging Findings of Vascular Lesions in The Head and NeckSLMC-QC IRNo ratings yet
- 10 1111@his 13961Document6 pages10 1111@his 13961DH SiriruiNo ratings yet
- Mass-Like Extramedullary Hematopoiesis: Imaging Features: Scientific ArticleDocument6 pagesMass-Like Extramedullary Hematopoiesis: Imaging Features: Scientific ArticleVo VũNo ratings yet
- Nodules Arising Within Port-Wine Stains: A Clinicopathologic Study of 31 CasesDocument8 pagesNodules Arising Within Port-Wine Stains: A Clinicopathologic Study of 31 CasesMichael Gaona LopezNo ratings yet
- Arteriovenous Malformations of The Body and Extremities: Analysis of Therapeutic Outcomes andDocument12 pagesArteriovenous Malformations of The Body and Extremities: Analysis of Therapeutic Outcomes andClaudio SalazarNo ratings yet
- Direct Evidence of Endothelial Injury in Acute Myocardial Infarction and Unstable Angina by Demonstration of Circulating Endothelial CellsDocument8 pagesDirect Evidence of Endothelial Injury in Acute Myocardial Infarction and Unstable Angina by Demonstration of Circulating Endothelial Cellsvalentina berrocal calderonNo ratings yet
- Orbital AVMDocument7 pagesOrbital AVMDedeh KurniasihNo ratings yet
- Genetics of Hemangiomas, Vascular Malformations, and Primary LymphedemDocument7 pagesGenetics of Hemangiomas, Vascular Malformations, and Primary LymphedemMiradz 'demmy' MuhidinNo ratings yet
- Preoperative Embolization of Cerebral Arteriovenous Malformations With OnyxDocument4 pagesPreoperative Embolization of Cerebral Arteriovenous Malformations With OnyxRifqi AnraNo ratings yet
- Article Zamboni BMJDocument9 pagesArticle Zamboni BMJfxchaserNo ratings yet
- Vascularized AmeloblastomaDocument5 pagesVascularized AmeloblastomaayuNo ratings yet
- Endovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDocument7 pagesEndovascular Management of Acute Epidural Hematomas: Clinical Experience With 80 CasesDeby AnditaNo ratings yet
- Asim, Prof-4500Document7 pagesAsim, Prof-4500Amina SidialiNo ratings yet
- OpenVetJ 13 233Document8 pagesOpenVetJ 13 233Emilia AmmariNo ratings yet
- X BibliDocument7 pagesX BibliBJ CarminatorNo ratings yet
- Intima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsDocument6 pagesIntima-Media Thickness of The Common Femoral Artery As A Marker of Leg Ulceration in Sickle Cell Disease PatientsAnonymous 9QxPDpNo ratings yet
- Medip,+1630 6396 1 CEDocument5 pagesMedip,+1630 6396 1 CEAvik singhNo ratings yet
- J Jstrokecerebrovasdis 2009 11 018Document6 pagesJ Jstrokecerebrovasdis 2009 11 018TriyanihzamNo ratings yet
- An Analysis of The Geometry of Saccular IntracraniDocument12 pagesAn Analysis of The Geometry of Saccular IntracraniAnnetNo ratings yet
- Composite Hemangioendothelioma An Unusual Presentation of A Rare Vascular TumorDocument5 pagesComposite Hemangioendothelioma An Unusual Presentation of A Rare Vascular TumorTian Nopita SariNo ratings yet
- SchwannomaDocument8 pagesSchwannomamit100792No ratings yet
- Connective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushDocument8 pagesConnective Tissue Diseases: Focus On Microcirculatory Bed: O.I. Zarudna, I.K. Venher, A.V. DovbushdjdNo ratings yet
- Articol ORLDocument6 pagesArticol ORLSabina BădilăNo ratings yet
- Cancer - 1 April 1991 - Ambros - MIC2 Is A Specific Marker For Ewing S Sarcoma and Peripheral Primitive NeuroectodermalDocument8 pagesCancer - 1 April 1991 - Ambros - MIC2 Is A Specific Marker For Ewing S Sarcoma and Peripheral Primitive NeuroectodermalAlba Yulieth Rodriguez NievesNo ratings yet
- Angiosarcoma of The Spleen: Imaging Characteristics in 12 PatientsDocument10 pagesAngiosarcoma of The Spleen: Imaging Characteristics in 12 PatientsHuyen NguyenNo ratings yet
- Warrier 2008Document3 pagesWarrier 2008darkmatter1No ratings yet
- Weissferdt 2015Document6 pagesWeissferdt 2015gabrielnunesNo ratings yet
- Hemangioendotelioma Epitelioide y Fusiforme de Ganglio Linfático. Caso ClínicoDocument4 pagesHemangioendotelioma Epitelioide y Fusiforme de Ganglio Linfático. Caso ClínicoMariana Duque GallegoNo ratings yet
- 0068KJR - KJR 20 1546Document8 pages0068KJR - KJR 20 1546Joshua AmenNo ratings yet
- Adeocarcinoma in Colonic Brushing CytologyDocument5 pagesAdeocarcinoma in Colonic Brushing CytologyCarl DonaireNo ratings yet
- JCTVS Myxo Ring Clinical Trial 2008Document9 pagesJCTVS Myxo Ring Clinical Trial 2008Nalini RajamannanNo ratings yet
- ShearWave Elastography Thyroid NodulesDocument8 pagesShearWave Elastography Thyroid Nodulesinfo8089No ratings yet
- Aneurysmal Bone CystDocument5 pagesAneurysmal Bone CystAustine OsaweNo ratings yet
- International 2Document4 pagesInternational 2daffunkmadansyahNo ratings yet
- Kim 2019Document7 pagesKim 2019Edison Chiriboga OrtegaNo ratings yet
- CT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingDocument9 pagesCT Angiography Versus Digital Subtraction Angiography For Intracranial Vascular Pathology in A Clinical SettingPari Pengda BaliNo ratings yet
- 1 s2.0 0735109788900940 MainDocument11 pages1 s2.0 0735109788900940 MainHarish SubramanianNo ratings yet
- (10920684 - Neurosurgical Focus) Cerebral Amyloid Angiopathy-Associated Intracerebral Hemorrhage - Pathology and ManagementDocument14 pages(10920684 - Neurosurgical Focus) Cerebral Amyloid Angiopathy-Associated Intracerebral Hemorrhage - Pathology and Managementkung_pauNo ratings yet
- Efficiency and Safety of Ethanol Sclerotherapy For Labial Arteriovenous MalformationsDocument9 pagesEfficiency and Safety of Ethanol Sclerotherapy For Labial Arteriovenous Malformationsradhianie djanNo ratings yet
- Modpathol 201783Document14 pagesModpathol 201783Tian Nopita SariNo ratings yet
- Norbash 99 AjnrDocument7 pagesNorbash 99 Ajnrthor112No ratings yet
- Angioleiomyoma in Soft Tissue of Extremities: MRI FindingsDocument4 pagesAngioleiomyoma in Soft Tissue of Extremities: MRI FindingsLuis Javier del PozoNo ratings yet
- 1 s2.0 S1933171109001302 MainDocument7 pages1 s2.0 S1933171109001302 MainRizky BafadhalNo ratings yet
- Carotid StentDocument9 pagesCarotid StentCut FadmalaNo ratings yet
- Pseudoanuerysms Made EasyDocument15 pagesPseudoanuerysms Made EasyFooffscribdNo ratings yet
- AVM CnsDocument31 pagesAVM CnsGamma KnifeNo ratings yet
- Colreavy 2000Document6 pagesColreavy 2000Yi-Hung SungNo ratings yet
- Epistaksis Dan TatalaksanaDocument4 pagesEpistaksis Dan TatalaksanametaferosiaNo ratings yet
- Cerebellar Hemangioblastoma-A Rare EntityDocument10 pagesCerebellar Hemangioblastoma-A Rare EntityJay LeheriNo ratings yet
- Jennette 1994Document6 pagesJennette 1994JOAO CARLOS BATISTA LIZNo ratings yet
- 3D Microvascular Architecture of Pre-Cancerous Lesions and Invasive Carcinomas of The ColonDocument9 pages3D Microvascular Architecture of Pre-Cancerous Lesions and Invasive Carcinomas of The ColonLuis Marin CalderónNo ratings yet
- Symptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and TreatmentDocument8 pagesSymptomatic Non-Stenotic Carotid Disease: Current Challenges and Opportunities For Diagnosis and Treatmentsnzbtk8df9No ratings yet
- Asensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Document12 pagesAsensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Edgar Geovanny Cardenas FigueroaNo ratings yet
- Cytogenetic Analysis in The Diagnosis of Acute Leukemia: Sverre Heim, FelixDocument9 pagesCytogenetic Analysis in The Diagnosis of Acute Leukemia: Sverre Heim, FelixEnas KharbotlyNo ratings yet
- Small Round Cell Tumors of Soft Tissue and BoneDocument13 pagesSmall Round Cell Tumors of Soft Tissue and BoneAdriana Gabriela Ugarte MacíasNo ratings yet
- Differentiation of Benign and Malignant Thyroid Nodules by Usin - 2018 - AcademiDocument10 pagesDifferentiation of Benign and Malignant Thyroid Nodules by Usin - 2018 - AcademiRicardo MirandaNo ratings yet
- Accepted Manuscript: 10.1016/j.wneu.2016.08.056Document6 pagesAccepted Manuscript: 10.1016/j.wneu.2016.08.056Elisabeth TikalakaNo ratings yet
- Journal Reading 1Document7 pagesJournal Reading 1Intan MayangsariNo ratings yet
- Diagnosis of Blood and Bone Marrow DisordersFrom EverandDiagnosis of Blood and Bone Marrow DisordersSa A. WangNo ratings yet
- General Internal Medicine In-Training ObjectivesDocument18 pagesGeneral Internal Medicine In-Training ObjectiveshectorNo ratings yet
- Endocrinology In-Training ObjectivesDocument12 pagesEndocrinology In-Training ObjectiveshectorNo ratings yet
- U.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRDocument60 pagesU.S. Selected Practice Recommendations For Contraceptive Use, 2016 MMWRhectorNo ratings yet
- Gauthier 1992Document6 pagesGauthier 1992hectorNo ratings yet
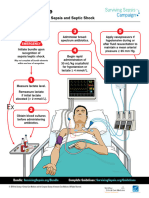
- Surviving Sepsis Campaign Hour 1 Bundle 220414 142741Document5 pagesSurviving Sepsis Campaign Hour 1 Bundle 220414 142741hectorNo ratings yet
- Metabolism With Triphasic Oral Contraceptive Formulations Containing Norgestimate or LevonorgestrelDocument6 pagesMetabolism With Triphasic Oral Contraceptive Formulations Containing Norgestimate or LevonorgestrelhectorNo ratings yet
- Episode ListDocument25 pagesEpisode ListhectorNo ratings yet
- Glasgow Coma Scale (With Explanations)Document1 pageGlasgow Coma Scale (With Explanations)hectorNo ratings yet
- Blood Pressure Log 02Document1 pageBlood Pressure Log 02hectorNo ratings yet
- Clinical Reasoning Guide FormDocument3 pagesClinical Reasoning Guide FormhectorNo ratings yet
- A Comparative Analysis of Three Methods of Contraception: Effects On Blood Glucose and Serum Lipid ProfilesDocument4 pagesA Comparative Analysis of Three Methods of Contraception: Effects On Blood Glucose and Serum Lipid ProfileshectorNo ratings yet
- ACGMECLERNational Report Findings 2019Document132 pagesACGMECLERNational Report Findings 2019hectorNo ratings yet
- Assignments Report: Saved ProgramsDocument16 pagesAssignments Report: Saved ProgramshectorNo ratings yet
- 060 Bonus LawOfCauseAndEffectDocument1 page060 Bonus LawOfCauseAndEffecthectorNo ratings yet
- 050 Bonus GratitudeDocument9 pages050 Bonus GratitudehectorNo ratings yet
- Fibromyalgia: Basic InformationDocument5 pagesFibromyalgia: Basic InformationhectorNo ratings yet
- Purpose, V Purpose, V Purpose, V Purpose, V Purpose, Vision, Ision, Ision, Ision, Ision, Goals Goals Goals Goals GoalsDocument9 pagesPurpose, V Purpose, V Purpose, V Purpose, V Purpose, Vision, Ision, Ision, Ision, Ision, Goals Goals Goals Goals GoalshectorNo ratings yet
- 056 Bonus RelativityDocument1 page056 Bonus RelativityhectorNo ratings yet
- The Law of Gender: Be Patient! All Ideas Move Into Form in The Right TimeDocument1 pageThe Law of Gender: Be Patient! All Ideas Move Into Form in The Right TimehectorNo ratings yet
- 008 ASereneMind PDFDocument2 pages008 ASereneMind PDFhectorNo ratings yet
- Cryotherapy: DR - Farah Mir Bugti (PT) 3/3/2021Document12 pagesCryotherapy: DR - Farah Mir Bugti (PT) 3/3/2021aza bellaNo ratings yet
- 2 Circulation SystemDocument29 pages2 Circulation SystemPERTUNIA KORABINo ratings yet
- Transport in AnimalsDocument43 pagesTransport in AnimalsEdwins MaranduNo ratings yet
- Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsDocument17 pagesCoronary Microvascular Disease Pathogenic Mechanisms and Therapeutic OptionsZuleynny TellesNo ratings yet
- NS 302 AnatomyDocument8 pagesNS 302 AnatomydhonaNo ratings yet
- Science: Modified Strategic Intervention MaterialsDocument42 pagesScience: Modified Strategic Intervention Materialsmichelle sumatNo ratings yet
- Nursing Care Plan: This Study Resource WasDocument6 pagesNursing Care Plan: This Study Resource WasCristina BernardoNo ratings yet
- Macroeconomics 9th Edition Boyes Test BankDocument25 pagesMacroeconomics 9th Edition Boyes Test BankMadisonKirbyeqko100% (54)
- Sickle Cell AnemiaDocument15 pagesSickle Cell AnemiakavitharavNo ratings yet
- Ebook Clinical Kinesiology and Anatomy 5Th Edition Lippert Test Bank Full Chapter PDFDocument25 pagesEbook Clinical Kinesiology and Anatomy 5Th Edition Lippert Test Bank Full Chapter PDFJeffreyLawsonmkbof100% (12)
- Mechanism of Inflammation (DRG Hesti) PPTDocument27 pagesMechanism of Inflammation (DRG Hesti) PPTTifani Cita DewiNo ratings yet
- Inhalational Nitric Oxide Systems - Part 1 - General Guidance On The Use of Inhaled Nitric OxideDocument12 pagesInhalational Nitric Oxide Systems - Part 1 - General Guidance On The Use of Inhaled Nitric OxidePSC PSCNo ratings yet
- Circulatory SystemDocument37 pagesCirculatory Systemcale suarezNo ratings yet
- Transport in Animals 4 QPDocument13 pagesTransport in Animals 4 QPRehan AhmadNo ratings yet
- Multiple Choice Questions (MCQ) Topic Quiz Cardiovascular SystemDocument19 pagesMultiple Choice Questions (MCQ) Topic Quiz Cardiovascular SystemMarimuthu ANo ratings yet
- Padhle 10th - Transportation (Life Processes) NotesDocument12 pagesPadhle 10th - Transportation (Life Processes) NotesNaitik AgrawalNo ratings yet
- Embolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewDocument20 pagesEmbolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewHai SheikhNo ratings yet
- Questions For ApmcDocument15 pagesQuestions For ApmcAde AlcarazNo ratings yet
- Laparoscopic SurgeryDocument4 pagesLaparoscopic SurgerycaioaccorsiNo ratings yet
- Prelox - A Patented Sexual Pleasure Enhancer - Fsponline-Recommends - Co.ukDocument18 pagesPrelox - A Patented Sexual Pleasure Enhancer - Fsponline-Recommends - Co.ukmihaiacNo ratings yet