You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lipoma and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasDocument8 pagesLipoma and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Free DHA Exam Online Practice Test With SolutionsDocument1 pageFree DHA Exam Online Practice Test With SolutionsShahnawaj AhmadNo ratings yet
- Pharmacology - Respiratory DrugsDocument61 pagesPharmacology - Respiratory DrugsBenjamin Joel Breboneria100% (5)
- How To Do Drug CalculationsDocument7 pagesHow To Do Drug Calculationsjk centralNo ratings yet
- AclsDocument73 pagesAclsKamel Hady50% (2)
- Paracetamol Drug StudyDocument1 pageParacetamol Drug StudyMaricor Toring85% (13)
- RanitidineDocument1 pageRanitidineliza sian100% (1)
- Laporan Jaga 7 AprileditDocument18 pagesLaporan Jaga 7 ApriledithansenNo ratings yet
- Adrenal Function: Adrenocorticotropic HormoneDocument11 pagesAdrenal Function: Adrenocorticotropic HormonehansenNo ratings yet
- 18e-Bcg Treatment SDocument2 pages18e-Bcg Treatment ShansenNo ratings yet
- Secondary Bsi 508Document77 pagesSecondary Bsi 508hansenNo ratings yet
- Fibromyalgia: An Update On Clinical Characteristics, Aetiopathogenesis and TreatmentDocument25 pagesFibromyalgia: An Update On Clinical Characteristics, Aetiopathogenesis and TreatmenthansenNo ratings yet
- Present Perfect Continuous and SimpleDocument3 pagesPresent Perfect Continuous and SimpleElena PradellNo ratings yet
- Persistence Market ResearchDocument8 pagesPersistence Market Researchapi-302003482No ratings yet
- Obat Keras N0vember 2021Document137 pagesObat Keras N0vember 2021antonNo ratings yet
- Brazil Resolution Re No 3385 13 Oct 2006Document4 pagesBrazil Resolution Re No 3385 13 Oct 2006Lackner MarceloNo ratings yet
- Drug Discovery - Drug Development LectureDocument6 pagesDrug Discovery - Drug Development LectureSkenzKenzNo ratings yet
- Flushing A Saline LockDocument30 pagesFlushing A Saline LockIvy SalcedoNo ratings yet
- Yang Betul PunyoDocument12 pagesYang Betul PunyoNor AzlinaNo ratings yet
- Public Perception and Behavior On The Disposal of Unused and Expired DrugsDocument12 pagesPublic Perception and Behavior On The Disposal of Unused and Expired DrugsMediterr J Pharm Pharm SciNo ratings yet
- Exposure and Response Prevention For Ocd SethDocument2 pagesExposure and Response Prevention For Ocd SethSofia nazeerNo ratings yet
- Stok Opnmae FixDocument6 pagesStok Opnmae FixRossa patria NandaNo ratings yet
- Topic 9. Non-Linear PKDocument17 pagesTopic 9. Non-Linear PKjoseNo ratings yet
- Discontinuing An IV InfusionDocument2 pagesDiscontinuing An IV InfusionNoel83% (6)
- Benzos Factsheet2011Document4 pagesBenzos Factsheet2011tech1322No ratings yet
- Daftar Obat Oral Padat Berdasarkan Kelas FarmakoterapiDocument3 pagesDaftar Obat Oral Padat Berdasarkan Kelas Farmakoterapigampang lupaNo ratings yet
- GALANG Mira Margarette v. PATIENT 5 Week 4 Day 1Document9 pagesGALANG Mira Margarette v. PATIENT 5 Week 4 Day 1Stiffany PrietoNo ratings yet
- Daftar Obat Alkes Trolley EmergencyDocument15 pagesDaftar Obat Alkes Trolley EmergencydevitaNo ratings yet
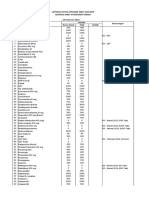
- Stock Obat Yang Akan Kadaluarsa 2020 NO Nama Item Satuan Prinsipal Harga Jual EDDocument4 pagesStock Obat Yang Akan Kadaluarsa 2020 NO Nama Item Satuan Prinsipal Harga Jual EDCorneLia JacintaNo ratings yet
- Good Manufacturing PracticeDocument3 pagesGood Manufacturing PracticeTinturulezNo ratings yet
- Guide Medprac Nurse DentistDocument14 pagesGuide Medprac Nurse DentistLukeNo ratings yet
- IFU Multipanel 5-10-12 Drogas Placas Monlabtest ENDocument2 pagesIFU Multipanel 5-10-12 Drogas Placas Monlabtest ENandrianzNo ratings yet
- Stock Obat & BHP PKM Ngadi-28 Feb 2021Document3 pagesStock Obat & BHP PKM Ngadi-28 Feb 2021Stela JoelNo ratings yet
- BPharm CurriculumDocument1 pageBPharm CurriculumMOHAMMED MNo ratings yet
- Pharmacodynamic Interactions of Amlodipine and Enalapril With Glyburide in Normal and Diseased RatsDocument28 pagesPharmacodynamic Interactions of Amlodipine and Enalapril With Glyburide in Normal and Diseased RatsKONDALREDDY JANNAPALLYNo ratings yet