You might also like
- Antipsychotics Factsheet pg2Document1 pageAntipsychotics Factsheet pg2JUSASBNo ratings yet
- Drugs To Watch With WARFARINDocument3 pagesDrugs To Watch With WARFARINRajendra RaiNo ratings yet
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- Insulin Chart: Insulin Type Onset of Action Peak Duration of ActionDocument1 pageInsulin Chart: Insulin Type Onset of Action Peak Duration of ActionGeorge ZachariahNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- Jurnal BioadhesifDocument10 pagesJurnal BioadhesifIzhal StewartNo ratings yet
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumNo ratings yet
- Transes PharmacodynamicsDocument36 pagesTranses PharmacodynamicsGwyneth Koleen Lopez100% (1)
- To Study The Effect of Various Tranquilizers and Sedatives On Motor Co-Ordination by Rotarod Test in Mice PDFDocument2 pagesTo Study The Effect of Various Tranquilizers and Sedatives On Motor Co-Ordination by Rotarod Test in Mice PDFSuman DahalNo ratings yet
- Revellionz'19 - Second Year Question BankDocument114 pagesRevellionz'19 - Second Year Question BankRamNo ratings yet
- FA 2016 Step 1 - Reference ValuesDocument2 pagesFA 2016 Step 1 - Reference ValuesJUSASBNo ratings yet
- Tramadol OMSDocument39 pagesTramadol OMSFranco VairolettiNo ratings yet
- Half LifeDocument43 pagesHalf LifeMinal Nadeem100% (1)
- Warfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureDocument6 pagesWarfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureVimi GeorgeNo ratings yet
- PharmecogenomicsDocument21 pagesPharmecogenomicsRatan Ratan100% (1)
- 02 - Basic and Clinical Evaluation of New DrugsDocument1 page02 - Basic and Clinical Evaluation of New DrugsKeisha Dela Cerna100% (1)
- Principles of PharmacotherapyDocument40 pagesPrinciples of Pharmacotherapyjunitria13No ratings yet
- Antihistamines: Student Learning GoalsDocument45 pagesAntihistamines: Student Learning GoalsDaniel WangNo ratings yet
- All Other ClassificationsDocument6 pagesAll Other ClassificationsCorey100% (1)
- Intern Drug ListDocument5 pagesIntern Drug ListKenette Diane CantubaNo ratings yet
- Dosage Form DesignDocument7 pagesDosage Form DesignNICOLE ANGELIQUE M. DINOYNo ratings yet
- GPAT Pharmacology SyllabusDocument3 pagesGPAT Pharmacology Syllabuskumar HarshNo ratings yet
- Experimental Pharmacology (PDFDrive)Document168 pagesExperimental Pharmacology (PDFDrive)Priya MohiteNo ratings yet
- Flexilor RangeDocument31 pagesFlexilor RangekurutalaNo ratings yet
- Cardiovascular System: Antihypertensive DrugsDocument73 pagesCardiovascular System: Antihypertensive Drugsأمجد محمدNo ratings yet
- APHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDocument13 pagesAPHA-Chapter-34 - Patient Assessment Laboratory: REVIEW OF SYSTEMS - Physical Assessment, Vital Signs& ObservationsDrSamia El WakilNo ratings yet
- PV Physical Pharmaceutics 4th SemDocument82 pagesPV Physical Pharmaceutics 4th SemSejal ShirgaveNo ratings yet
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- DRUG Interactions of Veterinary ImportanceDocument8 pagesDRUG Interactions of Veterinary ImportanceSunil100% (1)
- Introduction To PharmacognosyDocument12 pagesIntroduction To PharmacognosyReyes MesshaelNo ratings yet
- Cumulative Quiz 1: Calculate Dosages, Concentrations & Therapeutic OutcomesDocument6 pagesCumulative Quiz 1: Calculate Dosages, Concentrations & Therapeutic OutcomesTony AnsahNo ratings yet
- Pharmacokinetics and Pharmacodynamics 40Document40 pagesPharmacokinetics and Pharmacodynamics 40Shoaib BiradarNo ratings yet
- Barbiturates: of Action of GABA. Independent of GABADocument10 pagesBarbiturates: of Action of GABA. Independent of GABAAvi WerdesheimNo ratings yet
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaNo ratings yet
- CNS DepressantsDocument69 pagesCNS DepressantsMicah Lou Calamba100% (1)
- Pharmacology overview and key conceptsDocument16 pagesPharmacology overview and key conceptscuolyNo ratings yet
- 1 - 2 Introduction of Phytochemisry IDocument20 pages1 - 2 Introduction of Phytochemisry IZNA EntertainmentNo ratings yet
- Past Exam PaperDocument5 pagesPast Exam PaperDavid Le50% (2)
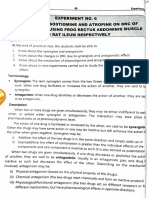
- Ex - Effect of Physostigmine and Atropine On DRCDocument9 pagesEx - Effect of Physostigmine and Atropine On DRCAryan Pisat100% (1)
- Posology 151223081101Document24 pagesPosology 151223081101eswarNo ratings yet
- Control of Drug Abuse and MisuseDocument40 pagesControl of Drug Abuse and MisuseMeena Ali100% (1)
- M. Pharm Review NAPLEX07Document1 pageM. Pharm Review NAPLEX07JUSASBNo ratings yet
- Antidepressants: HistoryDocument8 pagesAntidepressants: HistoryTejus Murthy A GNo ratings yet
- Practice ProblemsDocument2 pagesPractice ProblemsShemaj GurchumaNo ratings yet
- Chapter 6Document27 pagesChapter 6yeshi janexo100% (1)
- Receptor and Dose Response CurveDocument27 pagesReceptor and Dose Response Curveadnankhalid100% (2)
- Nanoparticles in Cancer Therapy and DiagnosisDocument55 pagesNanoparticles in Cancer Therapy and Diagnosismimshin0% (1)
- Introduction To Pharmacoepidemiology 2015 PDFDocument20 pagesIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapNo ratings yet
- Understanding PharmacologyDocument57 pagesUnderstanding Pharmacologyarun231187No ratings yet
- Opioid Analgesics - Narcotic Anlagesics - 0Document6 pagesOpioid Analgesics - Narcotic Anlagesics - 0Rajesh KumarNo ratings yet
- Drugs Interactions PDFDocument2 pagesDrugs Interactions PDFArne BorgerNo ratings yet
- Cholinergic ReceptorsDocument121 pagesCholinergic ReceptorsambroceNo ratings yet
- Prescribing Information For The Administration of AminophyllineDocument2 pagesPrescribing Information For The Administration of AminophyllinekolperrNo ratings yet
- Drug InteractionDocument2 pagesDrug InteractionNicole EncinaresNo ratings yet
- Phase-I Drug MetabolismDocument48 pagesPhase-I Drug MetabolismPhoebe LlameloNo ratings yet
- Top 10 Drug InteractionsDocument4 pagesTop 10 Drug InteractionsLeyla MajundaNo ratings yet
- ParacetamolDocument78 pagesParacetamolMichalNo ratings yet
- Oral Dispersible Tablets Novel Technology and Development PDFDocument7 pagesOral Dispersible Tablets Novel Technology and Development PDFHaider SalahNo ratings yet
- MUPAS, Grace Geraldine R. - Drug StudyDocument17 pagesMUPAS, Grace Geraldine R. - Drug StudyGrace Geraldine MupasNo ratings yet
- PharmacyDocument6 pagesPharmacyZehra AmirNo ratings yet
- Medicinal Chemistry-133Document4 pagesMedicinal Chemistry-133Zehra AmirNo ratings yet
- Med - Chem.Dept PC 810 Cardiovascular DrugsDocument45 pagesMed - Chem.Dept PC 810 Cardiovascular DrugsZehra AmirNo ratings yet
- Qatar Prometric MaterialsDocument170 pagesQatar Prometric MaterialsZehra Amir100% (1)
- NAPLEX Random Notes 68 PagesDocument51 pagesNAPLEX Random Notes 68 PagesZehra Amir100% (4)
- Applying For A Preregistration Pharmacist Post 2017 (2018 Intake)Document38 pagesApplying For A Preregistration Pharmacist Post 2017 (2018 Intake)Zehra AmirNo ratings yet
- Anti-Neoplastic Drugs PDFDocument19 pagesAnti-Neoplastic Drugs PDFZehra AmirNo ratings yet
- Cholinesterase Inhibitors2Document6 pagesCholinesterase Inhibitors2Zehra AmirNo ratings yet
- Anti-Psychotic Drugs PDFDocument10 pagesAnti-Psychotic Drugs PDFZehra AmirNo ratings yet
- Anti-Viral Drugs PDFDocument10 pagesAnti-Viral Drugs PDFZehra AmirNo ratings yet
- Cardiotonics & Inotropic Drugs PDFDocument10 pagesCardiotonics & Inotropic Drugs PDFZehra AmirNo ratings yet
- Cardiotonics & Inotropic Drugs PDFDocument10 pagesCardiotonics & Inotropic Drugs PDFZehra AmirNo ratings yet
- Cholinesterase Inhibitors2Document6 pagesCholinesterase Inhibitors2Zehra AmirNo ratings yet
- Narcotic Analgesics PDFDocument13 pagesNarcotic Analgesics PDFZehra AmirNo ratings yet
- CNS Stimulants PDFDocument7 pagesCNS Stimulants PDFZehra AmirNo ratings yet
- Registration RulesDocument27 pagesRegistration RulesZehra AmirNo ratings yet
- Optimasi Formula Tablet Effervescent Dispersi Padat Meloksikam Menggunakan Desain FaktorialDocument5 pagesOptimasi Formula Tablet Effervescent Dispersi Padat Meloksikam Menggunakan Desain FaktorialShelly Tri UtamiNo ratings yet
- Adult Medicines I. Medicines: PAN Pharmaceutical and Nutritional Products INCDocument6 pagesAdult Medicines I. Medicines: PAN Pharmaceutical and Nutritional Products INCJoshua Kevin Carl Tabar-GolpeNo ratings yet
- Philippine National Formulary As of February 2019Document62 pagesPhilippine National Formulary As of February 2019kkabness101 YULNo ratings yet
- List Harga ObatDocument11 pagesList Harga Obatklinik girimukti medical centerNo ratings yet
- Nathandoctor CVDocument6 pagesNathandoctor CVapi-582458131No ratings yet
- Major Antimycobacterial Drugs for TuberculosisDocument35 pagesMajor Antimycobacterial Drugs for TuberculosisJunah SeninaNo ratings yet
- Module 5: Drug Education: A C National Service Training Program (NSTP 1) NSTP DepartmentDocument8 pagesModule 5: Drug Education: A C National Service Training Program (NSTP 1) NSTP DepartmentRhea May EspressionNo ratings yet
- Amphotericin BDocument14 pagesAmphotericin BJuan David BastidasNo ratings yet
- Drugs Used in AnaesthesiaDocument29 pagesDrugs Used in AnaesthesiaMohamed NasryNo ratings yet
- Sultrine Sultrine: Sulfadiazine Sulfamerazine Sulfamethazine Sulfadiazine Sulfamerazine SulfamethazineDocument3 pagesSultrine Sultrine: Sulfadiazine Sulfamerazine Sulfamethazine Sulfadiazine Sulfamerazine SulfamethazineFaith de Leon ♥100% (1)
- Managing Medication SafelyDocument30 pagesManaging Medication Safelyshubham solankiNo ratings yet
- ChemSex (From A Safety Perspective)Document4 pagesChemSex (From A Safety Perspective)Dominic Milton TrottNo ratings yet
- Colchicine TabletsDocument16 pagesColchicine TabletsSaket SharmaNo ratings yet
- BY Dr. S.Sivaprasad Associate Professor MNR College of PharmacyDocument11 pagesBY Dr. S.Sivaprasad Associate Professor MNR College of PharmacySiva PrasadNo ratings yet
- Liquids LabelDocument5 pagesLiquids LabelLlosa JuneNo ratings yet
- HallucinogensDocument57 pagesHallucinogensrmiciuk34No ratings yet
- Alzheimer’s Disease Drug Development Pipeline 2019 Phase 3Document5 pagesAlzheimer’s Disease Drug Development Pipeline 2019 Phase 3Arjun GoleNo ratings yet
- Interesting Facts About Drug-Herb Interaction, Herbal Medicine & Herbal SupplementsDocument1 pageInteresting Facts About Drug-Herb Interaction, Herbal Medicine & Herbal SupplementsJerome Delos ReyesNo ratings yet
- Morphine (Parenteral) Guide for Neonatal Analgesia and SedationDocument5 pagesMorphine (Parenteral) Guide for Neonatal Analgesia and SedationRanggaDyantoNo ratings yet
- List of Participants - Refresher Course - ARCP - October 2021Document16 pagesList of Participants - Refresher Course - ARCP - October 2021PRATIK CHAUHAN100% (1)
- Ferrous sulfate for anemiaDocument3 pagesFerrous sulfate for anemiafahadNo ratings yet
- Neurology revision-2015: Benztropine side effects & status epilepticus treatmentsDocument99 pagesNeurology revision-2015: Benztropine side effects & status epilepticus treatmentsPaz Vida100% (7)
- Abstractbook Reims2015Document72 pagesAbstractbook Reims2015Kani RapeeNo ratings yet
- Manish M. Aglawe: R E S U M EDocument4 pagesManish M. Aglawe: R E S U M EnikuNo ratings yet
- Evaluasi Kebijakan Pengendalian Mutu Obat Dengan Uji Ketersediaan HayatiDocument6 pagesEvaluasi Kebijakan Pengendalian Mutu Obat Dengan Uji Ketersediaan HayatiMuhammad AndryNo ratings yet
- Digoxin slows heart rate and improves heart functionDocument6 pagesDigoxin slows heart rate and improves heart functionZiedTrikiNo ratings yet
- 213 2022 Article 6065Document15 pages213 2022 Article 6065tino valenNo ratings yet
- Generic Menu CardDocument9 pagesGeneric Menu CardLode DeocadesNo ratings yet
- Daivonex Ointment: Consumer Medicine InformationDocument7 pagesDaivonex Ointment: Consumer Medicine InformationAsh mohamedNo ratings yet
- 02-10-2022 Lista de PreciosDocument18 pages02-10-2022 Lista de PreciosIssac CoelloNo ratings yet