You might also like
- Purnama 2019 J. Phys. Conf. Ser. 1201 012048Document9 pagesPurnama 2019 J. Phys. Conf. Ser. 1201 012048Swaroop ChNo ratings yet
- Identification of Normal and Abnormal Ecg Using Neural NetworkDocument6 pagesIdentification of Normal and Abnormal Ecg Using Neural NetworkKani MozhiNo ratings yet
- Wang 2020 J. Phys. Conf. Ser. 1631 012073Document6 pagesWang 2020 J. Phys. Conf. Ser. 1631 012073Abduljabbar Salem Ba-MahelNo ratings yet
- Automatic Classification of Heartbeats Using Wavelet Neural NetworkDocument11 pagesAutomatic Classification of Heartbeats Using Wavelet Neural NetworkSamir GhoualiNo ratings yet
- Locating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised LearningDocument10 pagesLocating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised Learning施展No ratings yet
- Biomedical Signal Processing and Control: V. Mondéjar-Guerra, J. Novo, J. Rouco, M.G. Penedo, M. OrtegaDocument8 pagesBiomedical Signal Processing and Control: V. Mondéjar-Guerra, J. Novo, J. Rouco, M.G. Penedo, M. OrtegamuraliNo ratings yet
- 3830-Article Text-6888-1-10-20190701Document8 pages3830-Article Text-6888-1-10-20190701Marcell TakácsNo ratings yet
- Journal of ElectrocardiologyDocument7 pagesJournal of ElectrocardiologyAcho DoradoNo ratings yet
- Neural Networks in ECG ClassificationDocument36 pagesNeural Networks in ECG ClassificationMustafa AlkhzragyNo ratings yet
- Visvesvaraya Technological University Belagavi, Karnataka - 590 018Document3 pagesVisvesvaraya Technological University Belagavi, Karnataka - 590 018niranjan sNo ratings yet
- Cardiac Arrhythmia Detection Using Deep LearningDocument9 pagesCardiac Arrhythmia Detection Using Deep LearningRevati WableNo ratings yet
- A Fast Machine Learning Model For ECG-Based Heartbeat Classification and Arrhythmia DetectionDocument11 pagesA Fast Machine Learning Model For ECG-Based Heartbeat Classification and Arrhythmia DetectionAnita PalNo ratings yet
- Classification of Cardiovascular Disease Using Feature Extraction and Artificial Neural NetworksDocument16 pagesClassification of Cardiovascular Disease Using Feature Extraction and Artificial Neural NetworksmuraliNo ratings yet
- Deep Learning Algorithm For Arrhythmia Detection: Hilmy Assodiky, Iwan Syarif, Tessy BadriyahDocument7 pagesDeep Learning Algorithm For Arrhythmia Detection: Hilmy Assodiky, Iwan Syarif, Tessy BadriyahKani MozhiNo ratings yet
- Exploiting Similar Prior Knowledge For Compressing ECG SignalsDocument13 pagesExploiting Similar Prior Knowledge For Compressing ECG SignalsNaser MovahhediniaNo ratings yet
- David Et Al HeartrateDocument5 pagesDavid Et Al HeartrateDae Hyun BaikNo ratings yet
- Reviews: Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease ManagementDocument14 pagesReviews: Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease ManagementEdisonNo ratings yet
- Discriminating Electrocardiographic Responses To His-Bundle Pacing Using Machine LearningDocument10 pagesDiscriminating Electrocardiographic Responses To His-Bundle Pacing Using Machine LearningMaria AlejandraNo ratings yet
- Nature - Artificial Intelligence-Enhanced - 2021Document14 pagesNature - Artificial Intelligence-Enhanced - 2021Matheus Augusto Salerno Miguel e SousaNo ratings yet
- Classifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationDocument9 pagesClassifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationIAES IJAINo ratings yet
- Classification of Atrial Arrhythmias Using Neural Networks: IAES International Journal of Artificial Intelligence (IJ-AI)Document5 pagesClassification of Atrial Arrhythmias Using Neural Networks: IAES International Journal of Artificial Intelligence (IJ-AI)Jai UtkarshNo ratings yet
- Detection and Classification of Cardiac Arrhythmias by A Challenge-Best Deep Learning Neural Network ModelDocument27 pagesDetection and Classification of Cardiac Arrhythmias by A Challenge-Best Deep Learning Neural Network ModelMhd rdbNo ratings yet
- Brian 2017Document6 pagesBrian 2017Kani MozhiNo ratings yet
- REW4 Antennas AntennaMeasurements April19PDFDocument8 pagesREW4 Antennas AntennaMeasurements April19PDFEdenNo ratings yet
- 1 s2.0 S093336572200001X MainDocument11 pages1 s2.0 S093336572200001X MainNaila AshrafNo ratings yet
- Abdalla 2019Document9 pagesAbdalla 2019Bhargav KodaliNo ratings yet
- Research Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasetDocument11 pagesResearch Article: An Effective LSTM Recurrent Network To Detect Arrhythmia On Imbalanced ECG DatasettestNo ratings yet
- QRS Detection and Classification in Holter ECG Data in One Inference StepDocument9 pagesQRS Detection and Classification in Holter ECG Data in One Inference StepManh Hoang VanNo ratings yet
- Design of Low Power VLSI Architecture For Classification of Arrhythmic Beats Using DNN For Wearable Device ApplicationsDocument6 pagesDesign of Low Power VLSI Architecture For Classification of Arrhythmic Beats Using DNN For Wearable Device ApplicationsVaishnavi PanduranganNo ratings yet
- Carotida ComunDocument4 pagesCarotida ComunMariano DomanicoNo ratings yet
- Kwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using ElectrocardiographyDocument16 pagesKwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using Electrocardiography施展No ratings yet
- Entropy: CNN-FWS: A Model For The Diagnosis of Normal and Abnormal ECG With Feature AdaptiveDocument13 pagesEntropy: CNN-FWS: A Model For The Diagnosis of Normal and Abnormal ECG With Feature Adaptivejaviera.quirozNo ratings yet
- Detection and Classification of Arrhythmia Using An Explainable Deep Learning ModelDocument9 pagesDetection and Classification of Arrhythmia Using An Explainable Deep Learning ModelComisión Académica FCM - UNAHNo ratings yet
- Performance Evaluation of HRV Parameter Based Deep Neural NetworkDocument4 pagesPerformance Evaluation of HRV Parameter Based Deep Neural NetworkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Zarei 2018Document11 pagesZarei 2018Swarnadip SahaNo ratings yet
- Arrhythmia Detection - A Machine Learning BasedDocument5 pagesArrhythmia Detection - A Machine Learning BasedRyan Azmi Zuhdi DamanikNo ratings yet
- 2009 - Guillem - How Many Leads Are Necessary For A Reliable Reconstruction of AF ActivityDocument11 pages2009 - Guillem - How Many Leads Are Necessary For A Reliable Reconstruction of AF ActivitybamarcliNo ratings yet
- Entropy 23 00119Document13 pagesEntropy 23 00119Firas KACHROUDINo ratings yet
- Biomedical Signal Processing and ControlDocument10 pagesBiomedical Signal Processing and ControlSERGIO ANDRES ROMERO TORRESNo ratings yet
- Design and Evaluation of A Diaphragm For Electrocardiography in Eelectronic StethoscopesDocument8 pagesDesign and Evaluation of A Diaphragm For Electrocardiography in Eelectronic StethoscopesbellaNo ratings yet
- Arrhythmia Recognition and Classification Using Combined Parametric and Visual Pattern Features of ECG MorphologyDocument15 pagesArrhythmia Recognition and Classification Using Combined Parametric and Visual Pattern Features of ECG MorphologyAhmed AlrefaiNo ratings yet
- Deteksi Qrs Komplek Pada Pembacaan Heart Rate Variability (Metode TwoDocument12 pagesDeteksi Qrs Komplek Pada Pembacaan Heart Rate Variability (Metode TwoAyu NissaNo ratings yet
- Acharya 2017testDocument9 pagesAcharya 2017testALEX FERNANDO PEÑALOZA PILLCONo ratings yet
- 1 s2.0 S1746809421004407 MainDocument8 pages1 s2.0 S1746809421004407 MainAbdul WadudNo ratings yet
- Shoaib Healthcomm 2011Document6 pagesShoaib Healthcomm 2011HosseinNo ratings yet
- A Robust Deep Convolutional Neural Network With Batch - 2019 - Expert Systems WiDocument10 pagesA Robust Deep Convolutional Neural Network With Batch - 2019 - Expert Systems Wispike9444No ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Computers in Biology and Medicine: Yao Li, Qixun Qu, Meng Wang, Liheng Yu, Jun Wang, Linghao Shen, Kunlun HeDocument6 pagesComputers in Biology and Medicine: Yao Li, Qixun Qu, Meng Wang, Liheng Yu, Jun Wang, Linghao Shen, Kunlun Hevinoth muruganNo ratings yet
- 10.1016@S0140 67361931721 0Document7 pages10.1016@S0140 67361931721 0Oana DrăganNo ratings yet
- Lossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoDocument6 pagesLossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoOsamaNo ratings yet
- Lossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoDocument6 pagesLossy Compression Techniques For EEG Signals: Phuong Thi Dao, Xue Jun Li Hung Ngoc DoOsamaNo ratings yet
- Arrhy HD ResearchPaperDocument25 pagesArrhy HD ResearchPaperidesign whatNo ratings yet
- Accepted Manuscript: Computers in Biology and MedicineDocument21 pagesAccepted Manuscript: Computers in Biology and Medicinemuhammad sajidNo ratings yet
- Neural Networks Key To Improve EcgDocument10 pagesNeural Networks Key To Improve Ecgshivani1275No ratings yet
- Two Dimensional ECG Based Cardiac Arrhythmia Classification Using DSE ResNetDocument13 pagesTwo Dimensional ECG Based Cardiac Arrhythmia Classification Using DSE ResNetManh Hoang VanNo ratings yet
- Comparing Feature-Based Classifiers and Convolutional Neural Networks To Detect Arrhythmia From Short Segments of ECGDocument4 pagesComparing Feature-Based Classifiers and Convolutional Neural Networks To Detect Arrhythmia From Short Segments of ECGMhd rdbNo ratings yet
- Robust Classification of Cardiac Arrhythmia Using Machine LearningDocument9 pagesRobust Classification of Cardiac Arrhythmia Using Machine LearningIJRASETPublicationsNo ratings yet
- Cardiac Electrophysiology Without FluoroscopyFrom EverandCardiac Electrophysiology Without FluoroscopyRiccardo ProiettiNo ratings yet
- ECG Signal Processing, Classification and Interpretation: A Comprehensive Framework of Computational IntelligenceFrom EverandECG Signal Processing, Classification and Interpretation: A Comprehensive Framework of Computational IntelligenceNo ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- Nadi Astrology ResearchDocument6 pagesNadi Astrology ResearchAdvaitNo ratings yet
- Notes On Types of NadiDocument4 pagesNotes On Types of NadiAdvaitNo ratings yet
- FreeStyle Libre Pro Patient BrochureDocument2 pagesFreeStyle Libre Pro Patient BrochureAdvaitNo ratings yet
- Bharini NakshatraDocument1 pageBharini NakshatraAdvaitNo ratings yet
- Krittika NakshatraDocument2 pagesKrittika NakshatraAdvaitNo ratings yet
- Nadi AstrologyDocument7 pagesNadi AstrologyAdvaitNo ratings yet
- Nakshtra ResearchDocument7 pagesNakshtra ResearchAdvaitNo ratings yet
- This Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The Download .Ha Ha Ha This Line Is Added To Make Chutiya Out of ScribeDocument1 pageThis Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The Download .Ha Ha Ha This Line Is Added To Make Chutiya Out of ScribeAdvaitNo ratings yet
- Ashwini NakshatraDocument1 pageAshwini NakshatraAdvaitNo ratings yet
- Scribdchodu PDFDocument1 pageScribdchodu PDFAdvaitNo ratings yet
- This Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The DownloadDocument1 pageThis Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The DownloadAdvaitNo ratings yet
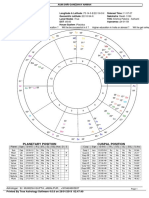
- VX Ge: Planetary Position Cuspal PositionDocument1 pageVX Ge: Planetary Position Cuspal PositionAdvaitNo ratings yet
- Hello PDFDocument1 pageHello PDFAdvaitNo ratings yet
- This Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The DownloadDocument1 pageThis Is Document Is Aimed To Make A Chutiya Out of Scribd .Enjoy The DownloadAdvaitNo ratings yet
- Effect of Chewing Tobacco On Fasting Blood Glucose LevelsDocument3 pagesEffect of Chewing Tobacco On Fasting Blood Glucose LevelsAdvaitNo ratings yet
- Linalg RefreshDocument3 pagesLinalg RefreshAdvaitNo ratings yet
- CSIC January 2018 Machine LearningDocument52 pagesCSIC January 2018 Machine LearningAdvaitNo ratings yet
- I Like Chutiya Banoing Very Much It Is My Fav Hobby I Like This Stuff Very Much As Much As I Like Anything ElseDocument1 pageI Like Chutiya Banoing Very Much It Is My Fav Hobby I Like This Stuff Very Much As Much As I Like Anything ElseAdvaitNo ratings yet
- Productflyer - 978 3 642 11709 1Document1 pageProductflyer - 978 3 642 11709 1AdvaitNo ratings yet
- CS 109: Data Science: Exploratory Data Analysis & Effective VisualizationsDocument99 pagesCS 109: Data Science: Exploratory Data Analysis & Effective VisualizationsAdvaitNo ratings yet
- Axis Bank Credit Card Important DetailsDocument23 pagesAxis Bank Credit Card Important DetailsAdvaitNo ratings yet
- Some Random ProjectDocument4 pagesSome Random ProjectAdvaitNo ratings yet
- ICICI Bank Credit Card Important DetailsDocument11 pagesICICI Bank Credit Card Important DetailsAdvaitNo ratings yet
- 07 Test ADocument24 pages07 Test ARashmin ShetNo ratings yet
- X16 42552VS2010UltimTrial1Document2 pagesX16 42552VS2010UltimTrial1An LcNo ratings yet
- Semi-Detailed Lesson Plan in TLE VIDocument3 pagesSemi-Detailed Lesson Plan in TLE VIPepper Santiago100% (5)
- Cheat Sheet - Mathematical Reasoning Truth Tables Laws: Conjunction: Double Negation LawDocument1 pageCheat Sheet - Mathematical Reasoning Truth Tables Laws: Conjunction: Double Negation LawVîñît YãdûvãñšhîNo ratings yet
- SIX SIGMA at GEDocument11 pagesSIX SIGMA at GE1987dezyNo ratings yet
- University of Khartoum Department of Electrical and Electronic Engineering Fourth YearDocument61 pagesUniversity of Khartoum Department of Electrical and Electronic Engineering Fourth YearMohamed AlserNo ratings yet
- On The Potential and Limits of (Global) Justice Through Law. A Frame of Research. Gianluigi PalombellaDocument12 pagesOn The Potential and Limits of (Global) Justice Through Law. A Frame of Research. Gianluigi Palombellaben zilethNo ratings yet
- Ielts Reading Test 10 - QuestionsDocument5 pagesIelts Reading Test 10 - QuestionsĐinh Quốc LiêmNo ratings yet
- Trainer Competency ModelDocument4 pagesTrainer Competency ModelpattapuNo ratings yet
- Third-Party LogisticsDocument16 pagesThird-Party Logisticsdeepshetty100% (1)
- 5 NopauseDocument95 pages5 NopauseLA garnerNo ratings yet
- Mahin Rahaman RESUMEDocument1 pageMahin Rahaman RESUMEMahin RahamanNo ratings yet
- Full HRM Notes by Ram Chad Ran SirDocument122 pagesFull HRM Notes by Ram Chad Ran SirKrupa PatilNo ratings yet
- 03 Task Performance 1 - ARG - MMW - RelevoDocument4 pages03 Task Performance 1 - ARG - MMW - Relevocessarine relevoNo ratings yet
- чек лист IELTS speaking September-December 2021Document2 pagesчек лист IELTS speaking September-December 2021Елена КуликоваNo ratings yet
- Lib Burst GeneratedDocument37 pagesLib Burst GeneratedIgnacio Del RioNo ratings yet
- Anilam 4200t CNC Programming and Operations ManualDocument355 pagesAnilam 4200t CNC Programming and Operations ManualAlexandru PrecupNo ratings yet
- Assignment 1 FRS651 Mac-July 2020Document2 pagesAssignment 1 FRS651 Mac-July 2020aizatNo ratings yet
- Current Trends On Syllabus Design PDFDocument5 pagesCurrent Trends On Syllabus Design PDFBosque AgujasNo ratings yet
- Medical AssistantDocument2 pagesMedical Assistantapi-78670766No ratings yet
- Motor Drives BY K .Sunil Kumar Griet-Power ElectronicsDocument4 pagesMotor Drives BY K .Sunil Kumar Griet-Power ElectronicsKalyan KumarNo ratings yet
- Types of EconomyDocument2 pagesTypes of EconomyAyush GargNo ratings yet
- American Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182Document5 pagesAmerican Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182JijoNo ratings yet
- PUP Manual EnglishDocument455 pagesPUP Manual EnglishCharo Pajuelo ChaskaNo ratings yet
- EXPATRIATESDocument38 pagesEXPATRIATESdsouzaa100% (2)
- Detailed Lesson PlanDocument7 pagesDetailed Lesson PlanMarjen MabasagNo ratings yet
- Ei GSM IcbDocument11 pagesEi GSM IcbwimaxaaabglNo ratings yet
- MotoSimEG-VRC Us PDFDocument816 pagesMotoSimEG-VRC Us PDFRafael SchroerNo ratings yet
- 3406 Discrete MathematicsDocument3 pages3406 Discrete MathematicsFaiza ShafiqNo ratings yet
- Understanding The Self Midterm Exam - PasigDocument1 pageUnderstanding The Self Midterm Exam - PasigEarl Tyrone P. Blanco100% (1)