You might also like
- 1BHK and 2BHK Cottage Floor Plans and Specifications from Rs. 25 LakhsDocument15 pages1BHK and 2BHK Cottage Floor Plans and Specifications from Rs. 25 Lakhsrajnish kumar100% (1)
- Thermal Imaging Camera t5 t6Document3 pagesThermal Imaging Camera t5 t6Arius GifeNo ratings yet
- ISO27k Guideline On ISMS Audit v2Document57 pagesISO27k Guideline On ISMS Audit v2Fredy AvilaNo ratings yet
- Electrocardiography Method (ECG/EKG): A Primary Guideline for Starters to Understand about Arrhythmias & EKG InterpretationFrom EverandElectrocardiography Method (ECG/EKG): A Primary Guideline for Starters to Understand about Arrhythmias & EKG InterpretationNo ratings yet
- Cardiac Arrhythmia Detection Using Deep LearningDocument9 pagesCardiac Arrhythmia Detection Using Deep LearningRevati WableNo ratings yet
- Electronics: Multiclass ECG Signal Analysis Using Global Average-Based 2-D Convolutional Neural Network ModelingDocument29 pagesElectronics: Multiclass ECG Signal Analysis Using Global Average-Based 2-D Convolutional Neural Network ModelingHoàng MạnhNo ratings yet
- sensors-21-06966-v3Document19 pagessensors-21-06966-v3Houichette AmiraNo ratings yet
- Classifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationDocument9 pagesClassifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationIAES IJAINo ratings yet
- Analysis of ECG Signals by Dynamic Mode DecompositionDocument12 pagesAnalysis of ECG Signals by Dynamic Mode Decompositionmadhumita mishraNo ratings yet
- Locating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised LearningDocument10 pagesLocating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised Learning施展No ratings yet
- 1 s2.0 S093336572200001X MainDocument11 pages1 s2.0 S093336572200001X MainNaila AshrafNo ratings yet
- Robust Classification of Cardiac Arrhythmia Using Machine LearningDocument9 pagesRobust Classification of Cardiac Arrhythmia Using Machine LearningIJRASETPublicationsNo ratings yet
- Implementation of A Portable Device For Real-Time ECG Signal AnalysisDocument13 pagesImplementation of A Portable Device For Real-Time ECG Signal AnalysisArham SheikhNo ratings yet
- Heart Rate MonitoringDocument3 pagesHeart Rate MonitoringJournalNX - a Multidisciplinary Peer Reviewed JournalNo ratings yet
- A Proposal For Monitoring Patients With Heart Failure Via "Smart Phone Technology "-Based ElectrocardiogramsDocument8 pagesA Proposal For Monitoring Patients With Heart Failure Via "Smart Phone Technology "-Based ElectrocardiogramsGabriella CsernákNo ratings yet
- Reviews: Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease ManagementDocument14 pagesReviews: Artificial Intelligence-Enhanced Electrocardiography in Cardiovascular Disease ManagementEdisonNo ratings yet
- Arm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotDocument9 pagesArm and Wrist Surface Potential Mapping For Wearable ECG Rhythm Recording Devices A PilotKarthik Raj VNo ratings yet
- Detection_of_Abnormal_Electrocardiogram_ECG_Using_Wavelet_Decomposition_and_Support_Vector_Machine_SVMDocument8 pagesDetection_of_Abnormal_Electrocardiogram_ECG_Using_Wavelet_Decomposition_and_Support_Vector_Machine_SVM20ee01045No ratings yet
- Entropy 23 00119Document13 pagesEntropy 23 00119Firas KACHROUDINo ratings yet
- Nature - Artificial Intelligence-Enhanced - 2021Document14 pagesNature - Artificial Intelligence-Enhanced - 2021Matheus Augusto Salerno Miguel e SousaNo ratings yet
- Detection of Abnormal Electrocardiogram (ECG) Using Wavelet Decomposition and Support Vector Machine (SVM)Document9 pagesDetection of Abnormal Electrocardiogram (ECG) Using Wavelet Decomposition and Support Vector Machine (SVM)NuruddinEmonNo ratings yet
- Jurnal EkgDocument26 pagesJurnal EkgUsman ohorellaNo ratings yet
- Biomedical Signal Processing and ControlDocument10 pagesBiomedical Signal Processing and ControlSERGIO ANDRES ROMERO TORRESNo ratings yet
- Development and Evaluation of Multilead PDFDocument10 pagesDevelopment and Evaluation of Multilead PDFfelixsafar3243No ratings yet
- Classification of ECG Signal Using FFT Based ImproDocument22 pagesClassification of ECG Signal Using FFT Based ImproHải LêNo ratings yet
- Mobile ECG Monitoring Device With Bioimpedance Measurement and AnalysisDocument7 pagesMobile ECG Monitoring Device With Bioimpedance Measurement and AnalysisShruti ShreeNo ratings yet
- Detection and Classification of Arrhythmia Using An Explainable Deep Learning ModelDocument9 pagesDetection and Classification of Arrhythmia Using An Explainable Deep Learning ModelComisión Académica FCM - UNAHNo ratings yet
- Simulation of ECG Instrumentation ECG Signal Using Advanced Instrumentation System Based On LAB Advanced Virtual Lab ViewDocument6 pagesSimulation of ECG Instrumentation ECG Signal Using Advanced Instrumentation System Based On LAB Advanced Virtual Lab ViewSitara KhanNo ratings yet
- Cardiogan: Attentive Generative Adversarial Network With Dual Discriminators For Synthesis of Ecg From PPGDocument9 pagesCardiogan: Attentive Generative Adversarial Network With Dual Discriminators For Synthesis of Ecg From PPGHala MostafaNo ratings yet
- Entropy: CNN-FWS: A Model For The Diagnosis of Normal and Abnormal ECG With Feature AdaptiveDocument13 pagesEntropy: CNN-FWS: A Model For The Diagnosis of Normal and Abnormal ECG With Feature Adaptivejaviera.quirozNo ratings yet
- 2010 Ieee Titb OreskoDocument7 pages2010 Ieee Titb OreskoPedro ContrerasNo ratings yet
- Tobej 4 217Document7 pagesTobej 4 217Rahmah Nida MurbahNo ratings yet
- Stages-Based ECG Signal Analysis From Traditional Signal Processing To Machine Learning Approaches A SurveyDocument22 pagesStages-Based ECG Signal Analysis From Traditional Signal Processing To Machine Learning Approaches A SurveyAzahel RangelNo ratings yet
- Jiang 2022 J. Phys. Conf. Ser. 2181 012055Document5 pagesJiang 2022 J. Phys. Conf. Ser. 2181 012055محمد عبدالحميد القرشيNo ratings yet
- Wang 2020 J. Phys. Conf. Ser. 1631 012073Document6 pagesWang 2020 J. Phys. Conf. Ser. 1631 012073Abduljabbar Salem Ba-MahelNo ratings yet
- Zhanpengjin 2009Document4 pagesZhanpengjin 2009äBHïSHëK DHöTëNo ratings yet
- Electronics 09 00121Document15 pagesElectronics 09 00121praba821No ratings yet
- 4 PBDocument12 pages4 PBkhouloud pfeNo ratings yet
- DDMHSA Dual Deterministic ModelBased Heart Sound Analysis For Daily Life MonitoringSensorsDocument17 pagesDDMHSA Dual Deterministic ModelBased Heart Sound Analysis For Daily Life MonitoringSensorsfrancogarciaramirez1No ratings yet
- 292 1690 1 PBDocument6 pages292 1690 1 PBJay NanavatiNo ratings yet
- Heart Rate Monitoring and PQRST Detection Based On Graphical User Interface With MatlabDocument6 pagesHeart Rate Monitoring and PQRST Detection Based On Graphical User Interface With MatlabSebastian PerezNo ratings yet
- Physiological Signal Monitoring SystemDocument5 pagesPhysiological Signal Monitoring SystemBira VekNo ratings yet
- Automated Defective ECG Signal Detection Using MATLAB ApplicationsDocument10 pagesAutomated Defective ECG Signal Detection Using MATLAB ApplicationsKishore Kanna Ravi KumarNo ratings yet
- Design and Fabrication of A Low Cost Heart Monitor Using Reflectance PhotoplethysmogramDocument11 pagesDesign and Fabrication of A Low Cost Heart Monitor Using Reflectance Photoplethysmogrammiroslav.kosticNo ratings yet
- A 1.06-ΜW Smart ECG Processor in 65-Nm CMOSDocument11 pagesA 1.06-ΜW Smart ECG Processor in 65-Nm CMOSjyotiNo ratings yet
- Modified Electrode Placements For Measurement of Hemodynamic Parameters Using Impedance CardiographyDocument12 pagesModified Electrode Placements For Measurement of Hemodynamic Parameters Using Impedance CardiographysalemNo ratings yet
- Computers in Biology and Medicine: Yao Li, Qixun Qu, Meng Wang, Liheng Yu, Jun Wang, Linghao Shen, Kunlun HeDocument6 pagesComputers in Biology and Medicine: Yao Li, Qixun Qu, Meng Wang, Liheng Yu, Jun Wang, Linghao Shen, Kunlun Hevinoth muruganNo ratings yet
- Electrocardiogram and Phonocardiogram MoDocument11 pagesElectrocardiogram and Phonocardiogram Mo1C22 MUHAMMAD ARMANDONo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- REW4 Antennas AntennaMeasurements April19PDFDocument8 pagesREW4 Antennas AntennaMeasurements April19PDFEdenNo ratings yet
- MainDocument12 pagesMainbozasnachoNo ratings yet
- Detection of Borderline Mental Disorder On Electrocardiosignals Using EMDDocument4 pagesDetection of Borderline Mental Disorder On Electrocardiosignals Using EMDJohnsonNo ratings yet
- Sensors 21 07163 v2Document18 pagesSensors 21 07163 v2emrecan cincanNo ratings yet
- Design of An ECG Sensor Circuitry For Cardiovascular Disease DiagnosisDocument6 pagesDesign of An ECG Sensor Circuitry For Cardiovascular Disease DiagnosisLaalai LaalaiNo ratings yet
- Saini 2015Document8 pagesSaini 2015äBHïSHëK DHöTëNo ratings yet
- Statistical and Entropy Based Features Can Efficiently Detect - 2020 - Medical PDFDocument6 pagesStatistical and Entropy Based Features Can Efficiently Detect - 2020 - Medical PDFMichael WondemuNo ratings yet
- Running Head: SCREENING TEST 1Document11 pagesRunning Head: SCREENING TEST 1DONALDNo ratings yet
- Brian 2017Document6 pagesBrian 2017Kani MozhiNo ratings yet
- Clinical Usefulness of The EASI 12 LeadDocument10 pagesClinical Usefulness of The EASI 12 Leademergency earlyNo ratings yet
- Deep Learning Algorithm Classifies Heartbeat Events Based On Electrocardiogram SignalsDocument10 pagesDeep Learning Algorithm Classifies Heartbeat Events Based On Electrocardiogram Signalsaryelit velardesNo ratings yet
- Neural Networks Key To Improve EcgDocument10 pagesNeural Networks Key To Improve Ecgshivani1275No ratings yet
- Algortmia Basados en Tiempo RealDocument11 pagesAlgortmia Basados en Tiempo RealRafa LeónNo ratings yet
- Automatic Classification of Heartbeats Using Wavelet Neural NetworkDocument11 pagesAutomatic Classification of Heartbeats Using Wavelet Neural NetworkSamir GhoualiNo ratings yet
- The Specific Objectives of This Lesson Are ToDocument11 pagesThe Specific Objectives of This Lesson Are TobellaNo ratings yet
- Adaptive Deep Learning-Based Air Quality Prediction Model Using The Most Relevant Spatial-Temporal RelationsDocument14 pagesAdaptive Deep Learning-Based Air Quality Prediction Model Using The Most Relevant Spatial-Temporal RelationsbellaNo ratings yet
- Deep Air Learning Interpolation, PredictionDocument13 pagesDeep Air Learning Interpolation, PredictionbellaNo ratings yet
- A Procedure For The Optimization of Air Quality Monitoring NetworksDocument7 pagesA Procedure For The Optimization of Air Quality Monitoring NetworksbellaNo ratings yet
- Hydraulic Servo Motor SystemDocument5 pagesHydraulic Servo Motor SystembellaNo ratings yet
- Types of CompressorsDocument16 pagesTypes of CompressorsbellaNo ratings yet
- Spek InverterDocument4 pagesSpek InverterbellaNo ratings yet
- 2,5 KW Wind Turbin (6 Units) Asset LapanDocument4 pages2,5 KW Wind Turbin (6 Units) Asset LapanbellaNo ratings yet
- Anfis WeatherDocument6 pagesAnfis WeatherbellaNo ratings yet
- Pengaruh Bukaan Terhadap Pencahayaan Alami Dan Penghawaan Alami Pada Masjid Al Ahdhar BekasiDocument14 pagesPengaruh Bukaan Terhadap Pencahayaan Alami Dan Penghawaan Alami Pada Masjid Al Ahdhar BekasiSiti M SalehNo ratings yet
- Analysis of RAM (Reliability, Availability, Maintainability) Production of Electric Voltage From 48 V PV (Photovoltaic) at Pantai Baru Pandansimo, IndonesiaDocument9 pagesAnalysis of RAM (Reliability, Availability, Maintainability) Production of Electric Voltage From 48 V PV (Photovoltaic) at Pantai Baru Pandansimo, IndonesiabellaNo ratings yet
- A Review On Maintenance Strategies For PV Systems - Elsevier Enhanced Reader-DikompresiDocument25 pagesA Review On Maintenance Strategies For PV Systems - Elsevier Enhanced Reader-DikompresibellaNo ratings yet
- Application of Statistical Process Control Chart For Monitoring Electric Power Losses Through Transmission and Distribution SystemDocument7 pagesApplication of Statistical Process Control Chart For Monitoring Electric Power Losses Through Transmission and Distribution SystembellaNo ratings yet
- 240V Solar Installation DiagramDocument1 page240V Solar Installation DiagrambellaNo ratings yet
- Reliability Evaluation of Electric Power Generation Systems With Solar PowerDocument83 pagesReliability Evaluation of Electric Power Generation Systems With Solar PowerbellaNo ratings yet
- Fault Detection in Electric Power Systems Based On Control ChartsDocument18 pagesFault Detection in Electric Power Systems Based On Control ChartsbellaNo ratings yet
- Air Quality Measurement Based LearningDocument15 pagesAir Quality Measurement Based LearningbellaNo ratings yet
- Hybrid Wind and Solar Power Plant AnalysisDocument7 pagesHybrid Wind and Solar Power Plant AnalysisFulki Kautsar SNo ratings yet
- An Improved Preventive Maintenance Scheduling For A Photovoltaic Plant Under Environmental ConstraintsDocument34 pagesAn Improved Preventive Maintenance Scheduling For A Photovoltaic Plant Under Environmental ConstraintsbellaNo ratings yet
- GUIBONE - GRADE12 - Week6 Home Learning Plans2Document2 pagesGUIBONE - GRADE12 - Week6 Home Learning Plans2Gizellen GuiboneNo ratings yet
- d472 MosfetDocument6 pagesd472 MosfetHutanu GabrielNo ratings yet
- A Study of Consumer Satisfaction On After Sales Service of Electronic ProductsDocument37 pagesA Study of Consumer Satisfaction On After Sales Service of Electronic ProductsKaran VarmaNo ratings yet
- Norfolk SlidesCarnivalDocument39 pagesNorfolk SlidesCarnivalFarah Soufana0% (1)
- Reflective Report 3 - ME-T12324PWB-1 - Group 8Document8 pagesReflective Report 3 - ME-T12324PWB-1 - Group 8Xiao FengNo ratings yet
- Technical Specification - MCS LiteDocument6 pagesTechnical Specification - MCS LiteKrunoslavNo ratings yet
- Flujometro SierraDocument52 pagesFlujometro SierraCapacitacion TodocatNo ratings yet
- Monthly Statement: This Month's SummaryDocument4 pagesMonthly Statement: This Month's Summaryit proNo ratings yet
- 6 MP Indoor/Outdoor Fisheye IR IP CamerasDocument4 pages6 MP Indoor/Outdoor Fisheye IR IP CamerascarlosNo ratings yet
- The Android Arsenal - Dialogs - Spots Progress DialogDocument8 pagesThe Android Arsenal - Dialogs - Spots Progress DialogRudolfNo ratings yet
- Linear/Multiple Regression: Application & Sample Problems Coefficient of DeterminationDocument17 pagesLinear/Multiple Regression: Application & Sample Problems Coefficient of Determinationanderson100% (1)
- VMware Vsphere Hyper Visor For Free - Based On ESXiDocument7 pagesVMware Vsphere Hyper Visor For Free - Based On ESXiCeleste SchmidtNo ratings yet
- Syllabus Recruitment of Mangement TraineesDocument6 pagesSyllabus Recruitment of Mangement TraineesSujith DeepakNo ratings yet
- Concrete Square Tapered PolesDocument4 pagesConcrete Square Tapered PolesElias100% (1)
- Unit I Lesson 4 Computing The Variance of A Discrete Probability DistributionDocument23 pagesUnit I Lesson 4 Computing The Variance of A Discrete Probability DistributionKira MilestoneNo ratings yet
- Similar Car ScanDocument10 pagesSimilar Car ScanHarsh SladeNo ratings yet
- Technical - STWS-ECS-FCU-103 AND 104Document1 pageTechnical - STWS-ECS-FCU-103 AND 104Prakash RaoNo ratings yet
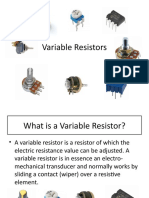
- Variable ResistorsDocument8 pagesVariable ResistorsKyle Brian Lacson EscarillaNo ratings yet
- Tsfluxus - g721 - enDocument38 pagesTsfluxus - g721 - enChris JonesNo ratings yet
- Unit V Processes and Operating SystemsDocument37 pagesUnit V Processes and Operating SystemsManikandan Annamalai100% (1)
- Significant Figures Worksheet - 1Document2 pagesSignificant Figures Worksheet - 1Yash ChauhanNo ratings yet
- Use Business TechnologyDocument35 pagesUse Business Technologyabricobm100% (3)
- Week 2Document4 pagesWeek 2Nam NguyenNo ratings yet
- Fortinet SMB Vs SonicWALL TZ Series - Talking PointsDocument2 pagesFortinet SMB Vs SonicWALL TZ Series - Talking PointsMonNo ratings yet
- FEM SyllabusDocument2 pagesFEM SyllabuscodieNo ratings yet
- Brochure2-Mobil Greases PDFDocument2 pagesBrochure2-Mobil Greases PDFPedro PerezNo ratings yet
- SHIDO LITHIUM BATTERY MANUALDocument4 pagesSHIDO LITHIUM BATTERY MANUALHIyer CARNo ratings yet