You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 3 Food Thyroid Boosting Daily ProtocolDocument22 pages3 Food Thyroid Boosting Daily Protocolpinkyhead99100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- EAI-02 OfficeDocument2 pagesEAI-02 OfficePeter Sare WolloNo ratings yet
- MSDS CNLITE Leaching ReagentDocument5 pagesMSDS CNLITE Leaching ReagentUrantuul dash100% (1)
- Laura Bruno The Lazy Raw Foodists GuideDocument192 pagesLaura Bruno The Lazy Raw Foodists Guideanatugario100% (1)
- Development of WalkingDocument13 pagesDevelopment of WalkingJudith Alexandra Castro GaeteNo ratings yet
- Cerebro - Cerebellar Circuits in Autism Spectrum DisorderDocument18 pagesCerebro - Cerebellar Circuits in Autism Spectrum DisorderJudith Alexandra Castro GaeteNo ratings yet
- Casual Relationship Between Malocclusion and Oral Muscles Dysfunction A Model of ApproachDocument3 pagesCasual Relationship Between Malocclusion and Oral Muscles Dysfunction A Model of ApproachJudith Alexandra Castro GaeteNo ratings yet
- Bjorl: Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionDocument6 pagesBjorl: Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionJudith Alexandra Castro GaeteNo ratings yet
- Postpartum Depression TheoryDocument9 pagesPostpartum Depression TheoryJan Oneille Y. Valles100% (1)
- Alternative TherapyDocument3 pagesAlternative Therapysohini bhattacharyaNo ratings yet
- Exposure To Mercury A Major Public Concern - WhoDocument5 pagesExposure To Mercury A Major Public Concern - WhoummuraraNo ratings yet
- Practice Giving Advice For These Problems: InstructionsDocument3 pagesPractice Giving Advice For These Problems: InstructionsMaier OlimpiuNo ratings yet
- Module 1 PATHFit1 Chapters 1 3Document46 pagesModule 1 PATHFit1 Chapters 1 3naomimarielleNo ratings yet
- Dr. Joel D. Wallach, Awarded 2011 Klaus Schwarz Commemorative Medal! Prestigious Scientific Award Recognizes Discovery of Selenium-Cystic Fibrosis LinkDocument3 pagesDr. Joel D. Wallach, Awarded 2011 Klaus Schwarz Commemorative Medal! Prestigious Scientific Award Recognizes Discovery of Selenium-Cystic Fibrosis LinkLawrence NapoleonNo ratings yet
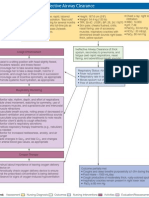
- Concept Map: Ineffective Airway ClearanceDocument1 pageConcept Map: Ineffective Airway ClearanceNikki Beverly G. BacaleNo ratings yet
- NHP 2018Document336 pagesNHP 2018Anonymous GULXxkXBNo ratings yet
- Every Child Matters and Teacher Education A UCET Position PaperDocument24 pagesEvery Child Matters and Teacher Education A UCET Position PaperAntonio PortelaNo ratings yet
- BilberryDocument13 pagesBilberrypepper100No ratings yet
- Case Study - DengueDocument28 pagesCase Study - DengueAlecs LunganNo ratings yet
- Tornwaldt's Cyst - Comments On Clinical CasesDocument3 pagesTornwaldt's Cyst - Comments On Clinical CasesPeertechz Publications Inc.No ratings yet
- Recommendations For Uniform Terminology in AnimalDocument10 pagesRecommendations For Uniform Terminology in AnimalNicolas VignoloNo ratings yet
- Jabulani Node Now Has A New Swimming Pool FinalDocument3 pagesJabulani Node Now Has A New Swimming Pool FinalJDANo ratings yet
- CV 2020 1Document5 pagesCV 2020 1Minerva Medical Treatment Pvt LtdNo ratings yet
- Group 5 Research Paper (Chapters 1 To 5)Document81 pagesGroup 5 Research Paper (Chapters 1 To 5)Rhison Asia100% (2)
- Spotter EmgDocument13 pagesSpotter EmgK Jayakumar KandasamyNo ratings yet
- The Impact of Gender Discrimination in The Workplace To Employees Emotional Well BeingDocument54 pagesThe Impact of Gender Discrimination in The Workplace To Employees Emotional Well BeingJustine LopezNo ratings yet
- Born To Die. Witchcraft and Infanticide in Baruba CultureDocument18 pagesBorn To Die. Witchcraft and Infanticide in Baruba CultureIñaki RegueraNo ratings yet
- Tylenol OverdoseDocument9 pagesTylenol OverdoseTyler HempelNo ratings yet
- Pathfit - 1 SLM 1Document51 pagesPathfit - 1 SLM 1Ronalyn ArcillasNo ratings yet
- Format Pelaporan Vaksinasi Covid-19 PKM PinelengDocument291 pagesFormat Pelaporan Vaksinasi Covid-19 PKM PinelengAnsella KuamanoNo ratings yet
- WHLP Personal Development Week 8Document2 pagesWHLP Personal Development Week 8Xazerco Lax100% (1)
- Arcaya - Week 4 Written AssignmentDocument2 pagesArcaya - Week 4 Written AssignmentIlert Kliene Tantoy ArcayaNo ratings yet
- Articulo Prope - GastrointestinalDocument7 pagesArticulo Prope - GastrointestinalValeria Garcia QuijanoNo ratings yet
- 340B Waste, Fraud & AbuseDocument21 pages340B Waste, Fraud & Abuseshepard stewartNo ratings yet