You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- FRCPath Mock 2014 Model AnswersDocument29 pagesFRCPath Mock 2014 Model Answersmonday125No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 3 - BIO-Describe The Feedback Mechanisms Involved in Menstrual CycleDocument11 pages3 - BIO-Describe The Feedback Mechanisms Involved in Menstrual CycleCarlo ThornappleNo ratings yet
- Embryo ExamDocument28 pagesEmbryo Exammoha100% (2)
- Mcqs Prometric Exam For Nursing: A. by The Appearance of The External GenitaliaDocument96 pagesMcqs Prometric Exam For Nursing: A. by The Appearance of The External GenitaliaAyman MohamedNo ratings yet
- Science 10 The Endocrine SystemDocument4 pagesScience 10 The Endocrine SystemTO NT ONNo ratings yet
- Lesson Plan 2020-2021Document7 pagesLesson Plan 2020-2021MELIE BAGARESNo ratings yet
- Amali Sistem Endokrin No 11Document4 pagesAmali Sistem Endokrin No 11Aisyah AliNo ratings yet
- Biology Score: Chapter 9.0: Reproduction & DevelopmentDocument31 pagesBiology Score: Chapter 9.0: Reproduction & DevelopmentNJ 4lyfeNo ratings yet
- Handout MCNDocument124 pagesHandout MCNcarol_gigliotti24No ratings yet
- Human Reproduction Male Reproductive System: (Continued)Document11 pagesHuman Reproduction Male Reproductive System: (Continued)Meeta DeviNo ratings yet
- Bio f4 Endocrine SystemDocument6 pagesBio f4 Endocrine SystemE-SKUUL ACADEMYNo ratings yet
- Mock - 1 Paper - 2 Test Questions PDFDocument38 pagesMock - 1 Paper - 2 Test Questions PDFAjay GokulNo ratings yet
- Growth and DevelopmentDocument144 pagesGrowth and DevelopmentRanjana SharmaNo ratings yet
- 6.6 Hormones, Homeostasis and Reproduction: Essential Idea: Hormones Are Used When Signals Need To Be Widely DistributedDocument37 pages6.6 Hormones, Homeostasis and Reproduction: Essential Idea: Hormones Are Used When Signals Need To Be Widely DistributedImeeNo ratings yet
- SOP FOR HOT AIR OVEN - CLEANING, OPERATION & CALIBRATION OF HOT AIR OVEN - Research SOPDocument1 pageSOP FOR HOT AIR OVEN - CLEANING, OPERATION & CALIBRATION OF HOT AIR OVEN - Research SOPSohail SheikhNo ratings yet
- Directions: Choose The Letter of The Correct Answer. Write Your Answers On Your Answer SheetDocument6 pagesDirections: Choose The Letter of The Correct Answer. Write Your Answers On Your Answer SheetVianca Andyella BendoNo ratings yet
- AgNPs Paper 3Document9 pagesAgNPs Paper 3VILEOLAGOLDNo ratings yet
- Investigations in InfertilityDocument43 pagesInvestigations in InfertilityAviral KashyapNo ratings yet
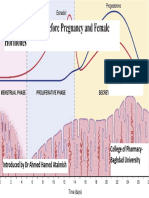
- Female Physiology Before Pregnancy and Female HormonesDocument13 pagesFemale Physiology Before Pregnancy and Female Hormonesمحمد رائد رزاق إسماعيلNo ratings yet
- Gynaecology Passmed PlabDocument49 pagesGynaecology Passmed PlabDoctor daveNo ratings yet
- Curs I MG 2017Document12 pagesCurs I MG 2017muresanf_5No ratings yet
- Acupuncture IVFDocument10 pagesAcupuncture IVFWolfgang Rb100% (1)
- Semen Quality Obesity PlusDocument23 pagesSemen Quality Obesity PlusPOPA EMILIANNo ratings yet
- Mark SchemeDocument140 pagesMark SchemeAnonymous khzvzZZfmjNo ratings yet
- Mapeh 8 Week 1 - 2Document11 pagesMapeh 8 Week 1 - 2JEAN ANN BACONGCO CAMITNo ratings yet
- Pituitary GlandDocument15 pagesPituitary GlandPutri Agustin Mere100% (1)
- Male Reproductive SystemDocument8 pagesMale Reproductive SystemShayu ShaNo ratings yet
- (Template) Lab Report TemplateDocument16 pages(Template) Lab Report TemplateArunima 620006No ratings yet
- Chapter-3. Human Reproduction Case Based QuestionsDocument33 pagesChapter-3. Human Reproduction Case Based QuestionsSania GeorgeNo ratings yet
- Hypothalamus and Pituitary GlandDocument62 pagesHypothalamus and Pituitary GlandphyMedza AppNo ratings yet