You might also like
- CNMC Eye OSPE Problems With SolutionsDocument26 pagesCNMC Eye OSPE Problems With SolutionsShahbaz AAnsariNo ratings yet
- part1Document15 pagespart1solimanmahmoudaNo ratings yet
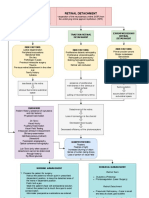
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Care For Patients With Alteration in Perception and CoordinationDocument12 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Red EyeDocument54 pagesRed EyeT786 kharNo ratings yet
- Glaucoma Diagnosis and TreatmentDocument47 pagesGlaucoma Diagnosis and Treatmentnurul ramadhiniNo ratings yet
- Post Test JWB NCLDocument12 pagesPost Test JWB NCLSummer SnowNo ratings yet
- Guide to Managing Common Ocular Trauma InjuriesDocument50 pagesGuide to Managing Common Ocular Trauma Injuriesaditya brahmantio sujakaNo ratings yet
- عملي السليداتDocument92 pagesعملي السليداتSandyDavidNo ratings yet
- 10 Lids and Lashes 2016Document13 pages10 Lids and Lashes 2016willemlrouxNo ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument5 pagesCorneal Dystrophies: Retinal DetachmentCake ManNo ratings yet
- Anatomy & Degenerations of Peripheral RetinaDocument29 pagesAnatomy & Degenerations of Peripheral RetinaNeelam Khatwani100% (1)
- SOPS For Blunt Trauma02Document2 pagesSOPS For Blunt Trauma02jawad awanNo ratings yet
- Tatalaksana GlaukomaDocument53 pagesTatalaksana GlaukomaVeronika Marampa AllolinggiNo ratings yet
- Angle Closure GlaucomaDocument21 pagesAngle Closure Glaucomasri sinagaNo ratings yet
- EGurukul - Uveitis and Uveal TractDocument10 pagesEGurukul - Uveitis and Uveal TractOscar Daniel MendezNo ratings yet
- Glaucoma 2 Lecture PACG MBBS BY Prof Munim SuriDocument28 pagesGlaucoma 2 Lecture PACG MBBS BY Prof Munim SuriMunim SuriNo ratings yet
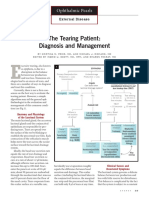
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- Case Bacterial KeratitisDocument44 pagesCase Bacterial KeratitisPagolu BavyaNo ratings yet
- ENT Trans Disorders of The External EarDocument4 pagesENT Trans Disorders of The External EarJared Ezrach Cacal SanidadNo ratings yet
- 27a. Retinal Disease 1Document44 pages27a. Retinal Disease 1Aa SsNo ratings yet
- Retinal Diseases George Pile, MD: RetinaDocument5 pagesRetinal Diseases George Pile, MD: RetinaPrincess Cate MercadoNo ratings yet
- Eyelids and Lacrimal ApparatusDocument6 pagesEyelids and Lacrimal Apparatussarguss14No ratings yet
- Ectropion and Corneal Ulcer CareDocument31 pagesEctropion and Corneal Ulcer CareapriliaNo ratings yet
- Surgery B PracticalDocument12 pagesSurgery B PracticalMohamed KhaledNo ratings yet
- GlaucomaDocument1 pageGlaucomashakyaNo ratings yet
- Materi Bimbingan Kepaniteraan Klinik Ilmu Penyakit Mata: No Pembimbing Topik Sub TopikDocument2 pagesMateri Bimbingan Kepaniteraan Klinik Ilmu Penyakit Mata: No Pembimbing Topik Sub TopikRizka ChairaniNo ratings yet
- Occupational Hazards in Dental, Textile Industry and MechanicDocument20 pagesOccupational Hazards in Dental, Textile Industry and MechanicimtahifNo ratings yet
- Referat Acute Liver FailureDocument124 pagesReferat Acute Liver FailurepanduNo ratings yet
- Medical History Taking Project Ppt-Converted NoDocument17 pagesMedical History Taking Project Ppt-Converted Noabdul qayyumNo ratings yet
- Cataract Surgery Complications GuideDocument130 pagesCataract Surgery Complications GuideMauVeeNo ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- Glaucoma: Camille N. LibrandaDocument35 pagesGlaucoma: Camille N. LibrandaCamilleNo ratings yet
- Corneal Dystrophies, Contact Lenses, and Retinal Detachment GuideDocument6 pagesCorneal Dystrophies, Contact Lenses, and Retinal Detachment GuideMarissa AsimNo ratings yet
- Roughtly: LayerDocument18 pagesRoughtly: LayerS SwaminathanNo ratings yet
- Ocular Emergencies GuideDocument7 pagesOcular Emergencies GuidePatricia ManaliliNo ratings yet
- 8a) Chronic DacryocystitisDocument5 pages8a) Chronic DacryocystitisDasNo ratings yet
- White dot syndromes: causes, signs and treatmentDocument43 pagesWhite dot syndromes: causes, signs and treatmentJasmine MinoNo ratings yet
- Common Eye Diseases 2022Document33 pagesCommon Eye Diseases 2022Shia LevyNo ratings yet
- Brain AbscessDocument3 pagesBrain AbscessAndrew JavierNo ratings yet
- EGurukul GlaucomaDocument15 pagesEGurukul GlaucomaOscar Daniel Mendez100% (1)
- Keratoconjunctivitis Sicca: in DogsDocument8 pagesKeratoconjunctivitis Sicca: in DogsGABRIELA VERGARA PEREZNo ratings yet
- Opt Halm OlogyDocument1 pageOpt Halm OlogyAnonymous q16bp7No ratings yet
- Ophthalmology EmergenciesDocument60 pagesOphthalmology Emergenciesasraf amirullahNo ratings yet
- The Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of OnsetDocument4 pagesThe Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of Onsetleigh_zaliNo ratings yet
- Ocular EmergencyDocument86 pagesOcular EmergencyMohammadNo ratings yet
- KeratoconusssDocument15 pagesKeratoconusssnurfatminsari almaidinNo ratings yet
- Orbita, Palpebra & Sistem Lakrimal: Dr. I Gede Suparta SP.MDocument43 pagesOrbita, Palpebra & Sistem Lakrimal: Dr. I Gede Suparta SP.Mbasyit bafadhalNo ratings yet
- Retinal Detachment SlideDocument54 pagesRetinal Detachment SlideHerin NataliaNo ratings yet
- Expansion With Excision: George Clooney Nasal Dorsum Length of Eye Angle of Mandible/jawDocument4 pagesExpansion With Excision: George Clooney Nasal Dorsum Length of Eye Angle of Mandible/jawChristine Evan HoNo ratings yet
- Dermatology Revision E6.5 'Document35 pagesDermatology Revision E6.5 'Riya SharmaNo ratings yet
- Fundamentals of OpthalmologyDocument4 pagesFundamentals of OpthalmologyMuhammad HaziqNo ratings yet
- Pediatrics2 Se4 High2Document23 pagesPediatrics2 Se4 High2Daryl Gay NanoNo ratings yet
- Papiledema 3Document27 pagesPapiledema 3nellieauthorNo ratings yet
- Opthalmology Visuals New PDF-1Document100 pagesOpthalmology Visuals New PDF-1singh0% (1)
- Eyes Lecture 2Document4 pagesEyes Lecture 2Rue Cheng MaNo ratings yet
- ConjunctivitisDocument4 pagesConjunctivitisKumar ShivamNo ratings yet
- Clinical Ophthalmology for UndergraduatesFrom EverandClinical Ophthalmology for UndergraduatesRating: 4 out of 5 stars4/5 (5)
- ASEAN Stability GuidelineDocument37 pagesASEAN Stability GuidelinevarizzzNo ratings yet
- Mock Claim Form 2Document2 pagesMock Claim Form 2Toni Sy EncinaresNo ratings yet
- Qualitative Test For Amino AcidsDocument1 pageQualitative Test For Amino AcidsToni Sy EncinaresNo ratings yet
- PhilHealth ClaimForm2 Guidelines PDFDocument8 pagesPhilHealth ClaimForm2 Guidelines PDFToni Sy EncinaresNo ratings yet
- Extraction of Lipids From Chicken Egg YolkDocument5 pagesExtraction of Lipids From Chicken Egg YolkToni Sy Encinares100% (2)
- Pharmacology Types of ReceptorsDocument2 pagesPharmacology Types of ReceptorsToni Sy EncinaresNo ratings yet
- Toxicology Qualitative TestDocument5 pagesToxicology Qualitative TestToni Sy EncinaresNo ratings yet
- Effect of PH On Invertase ActivityDocument4 pagesEffect of PH On Invertase ActivityToni Sy Encinares100% (2)
- Sythesization and Purification of Acetanilide by Acetylation and Re CrystallizationDocument4 pagesSythesization and Purification of Acetanilide by Acetylation and Re CrystallizationToni Sy EncinaresNo ratings yet
- PCARE Calculation NotesDocument10 pagesPCARE Calculation NotesToni Sy EncinaresNo ratings yet
- Determination of Ethanol Content From Ginebra Gin by Fractional DistillationDocument4 pagesDetermination of Ethanol Content From Ginebra Gin by Fractional DistillationToni Sy EncinaresNo ratings yet
- NCP&SOAPIEDocument4 pagesNCP&SOAPIEMica OmotsosircNo ratings yet
- Cosmecueticals Mod1Document35 pagesCosmecueticals Mod1Top 10No ratings yet
- Continued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyDocument10 pagesContinued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyMichele MarengoNo ratings yet
- Drug study overviewDocument3 pagesDrug study overvieweliza luisNo ratings yet
- Fordyce GranuleDocument3 pagesFordyce GranulenediaNo ratings yet
- Abu Dhabi Plan Drug ListDocument45 pagesAbu Dhabi Plan Drug ListicebreakNo ratings yet
- Danile Fast BrochureDocument2 pagesDanile Fast BrochureLito Dela PeñaNo ratings yet
- Clinical Nutrition General BrochureDocument40 pagesClinical Nutrition General Brochureds.neetaNo ratings yet
- Factors Affecting Body Alignment & Activity 1. 2. 3.Document5 pagesFactors Affecting Body Alignment & Activity 1. 2. 3.LE-JEAN BRENA100% (2)
- Ketamine Administration Guideline 080114 راهنماDocument14 pagesKetamine Administration Guideline 080114 راهنماBabak AsliNo ratings yet
- Septage FAQ Brochure - EnglishDocument2 pagesSeptage FAQ Brochure - EnglishMeghan EbuezaNo ratings yet
- Shell Tellus S2 MX 68: Safety Data SheetDocument16 pagesShell Tellus S2 MX 68: Safety Data SheettinaseNo ratings yet
- cp201007 Spotlight Febuxostat-261Document2 pagescp201007 Spotlight Febuxostat-261Rafaeyza Al KarimNo ratings yet
- Ethics Documents For Physio TherapistsDocument21 pagesEthics Documents For Physio TherapistsDeeksha JainNo ratings yet
- Elyse Torres Resume NowDocument2 pagesElyse Torres Resume Nowapi-395806896No ratings yet
- Ocular InjuryDocument46 pagesOcular InjurysnyNo ratings yet
- Bedbug Propoxur LabelDocument3 pagesBedbug Propoxur LabeluncleadolphNo ratings yet
- Vacuum PumpDocument90 pagesVacuum PumpEnrique S OcampoNo ratings yet
- Dipyridamole Tablets Leaflet SectionsDocument1 pageDipyridamole Tablets Leaflet SectionsAat Prayoga MuhtarNo ratings yet
- Resume March2023Document2 pagesResume March2023api-625227498No ratings yet
- CBT of DepressionDocument15 pagesCBT of DepressionRidwan MuttaqinNo ratings yet
- Complementary and Alternative TherapyDocument16 pagesComplementary and Alternative TherapyDevangi Bhorsat100% (1)
- Sample EssayDocument9 pagesSample EssayBrian SrotaNo ratings yet
- State Apple Health Handbook PDFDocument28 pagesState Apple Health Handbook PDFRohan KunwerNo ratings yet
- The Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesDocument10 pagesThe Efficacy of Mechanical Vibration Analgesia For Relief of Heel Stick Pain in NeonatesmustafasacarNo ratings yet
- Effect of Micronutrients and Organics on Baby Corn-Chickpea YieldDocument3 pagesEffect of Micronutrients and Organics on Baby Corn-Chickpea YieldRitesh MistryNo ratings yet
- Pterygium: Surgical Techniques and ChoicesDocument2 pagesPterygium: Surgical Techniques and ChoicesJohny Marquez TrochezNo ratings yet
- Ayurvedic treatment of anemia in pregnancyDocument6 pagesAyurvedic treatment of anemia in pregnancypooja huilgolNo ratings yet
- 1-Collection, Storage and Transportataion of MicrobiologicalDocument49 pages1-Collection, Storage and Transportataion of MicrobiologicalSummi NizNo ratings yet
- Manual Usuario (Enghlis) Babylog 8000 PlusDocument172 pagesManual Usuario (Enghlis) Babylog 8000 PlusJuan Carlos LopezNo ratings yet