You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Borderline Personality Disorder WorksheetsDocument2 pagesBorderline Personality Disorder WorksheetsHaryo WicaksonoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A319/A320/A321 Transit CheckDocument2 pagesA319/A320/A321 Transit CheckHiram ThomasNo ratings yet
- TB Guideline TreatmentDocument14 pagesTB Guideline TreatmentNovii NoviiNo ratings yet
- CarbetocinDocument9 pagesCarbetocinNovii NoviiNo ratings yet
- Idhe 2009 London Malnutrition Fenn PDFDocument90 pagesIdhe 2009 London Malnutrition Fenn PDFNovii NoviiNo ratings yet
- An Introduction To Corneal TransplantationDocument2 pagesAn Introduction To Corneal TransplantationNovii NoviiNo ratings yet
- 1 s2.0 S2214109X15002971Document2 pages1 s2.0 S2214109X15002971Novii NoviiNo ratings yet
- Pabc ScoreDocument4 pagesPabc ScoreNovii NoviiNo ratings yet
- Homeostasis, and The Contribution of Digestive System To HomeostasisDocument29 pagesHomeostasis, and The Contribution of Digestive System To HomeostasisNovii NoviiNo ratings yet
- CarbetocinDocument9 pagesCarbetocinNovii NoviiNo ratings yet
- Pain Aapa Rev8Document101 pagesPain Aapa Rev8Novii NoviiNo ratings yet
- Tecnix - FV REGULADOR PDFDocument2 pagesTecnix - FV REGULADOR PDFVICTORACARAPINo ratings yet
- Solicitation LetterDocument3 pagesSolicitation Letterapi-418550832No ratings yet
- Who Ca+Document32 pagesWho Ca+Douglas HagmannNo ratings yet
- IrrigationDocument19 pagesIrrigationpriya santosh nalamwarNo ratings yet
- Kangure Francis Mugo-PHD HRM-2014 PDFDocument204 pagesKangure Francis Mugo-PHD HRM-2014 PDFanushanNo ratings yet
- The Following Text Is For Questions Number 1 - 4!: Exercise On Greeting CardDocument2 pagesThe Following Text Is For Questions Number 1 - 4!: Exercise On Greeting CardnagaNo ratings yet
- Computational Fluid Dynamics Modeling of Cell Cultures in Bioreactors and Its Potential For Cultivated Meat Production - A Mini-ReviewDocument10 pagesComputational Fluid Dynamics Modeling of Cell Cultures in Bioreactors and Its Potential For Cultivated Meat Production - A Mini-ReviewArianna RechNo ratings yet
- Benefits of Enabled Gardening - Gardening For The HomelessDocument5 pagesBenefits of Enabled Gardening - Gardening For The HomelessNeroulidi854No ratings yet
- Development Agreement: Former Macy's HQDocument10 pagesDevelopment Agreement: Former Macy's HQWVXU NewsNo ratings yet
- SEBI Takeover Code NewDocument49 pagesSEBI Takeover Code Newtooryrizvi100% (1)
- CM692 Im6129 Yh135 PDFDocument90 pagesCM692 Im6129 Yh135 PDFmoises100% (1)
- 177 Mental ToughnessDocument3 pages177 Mental Toughnessmadan_adhikari100% (1)
- Shampoo BarDocument1 pageShampoo BarrezaNo ratings yet
- CH 9 ArticulationsDocument40 pagesCH 9 ArticulationsRobin ToneyNo ratings yet
- Conditions That Affect Cultural VariationDocument2 pagesConditions That Affect Cultural Variationtemujin0364% (14)
- Herbs by Sebastian DebskiDocument9 pagesHerbs by Sebastian DebskiYakuma HotaruNo ratings yet
- Sodium Laureth SulfateDocument2 pagesSodium Laureth Sulfatemarvin quitaNo ratings yet
- Earthquake Seismology & Plate Tectonic by Dr. Zulfiqar Ahmad NCPDocument75 pagesEarthquake Seismology & Plate Tectonic by Dr. Zulfiqar Ahmad NCPkazimmehdiNo ratings yet
- Botswana-Upenn Partnership: Basic SetswanaDocument10 pagesBotswana-Upenn Partnership: Basic SetswanakhumisoNo ratings yet
- Pre Seen Case Study For BM Paper 1 (HL & SL)Document5 pagesPre Seen Case Study For BM Paper 1 (HL & SL)Siddhant MaheshwariNo ratings yet
- QL40 CAL: 3 Arm CaliperDocument2 pagesQL40 CAL: 3 Arm Caliperum erNo ratings yet
- Effect of I Love You (ILU) Massage On Rehabilitation of Children Digestive Function Postoperative StomachDocument7 pagesEffect of I Love You (ILU) Massage On Rehabilitation of Children Digestive Function Postoperative StomachSufi NurkhairunnisaNo ratings yet
- Reading ComprehensionDocument14 pagesReading ComprehensionanwarofswatNo ratings yet
- Neurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"Document3 pagesNeurologist Deborah Boland, D.O., MSPT, Named "Physician of The Year"PR.comNo ratings yet
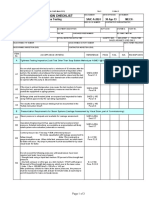
- SAIC-A-2024 Rev 6 Leakness Tightness TestDocument3 pagesSAIC-A-2024 Rev 6 Leakness Tightness Testpookkoya thangalNo ratings yet
- Emmanuel Torres CV.Document4 pagesEmmanuel Torres CV.Mathew Cedeño AvellanNo ratings yet
- 2 Workforce Safety and WellnessDocument124 pages2 Workforce Safety and Wellnessanmz09No ratings yet
- Chemical Composition and Industrial Characterization of The Dutsen Bundot Feldspars, Dass, Bauchi State, NigeriaDocument8 pagesChemical Composition and Industrial Characterization of The Dutsen Bundot Feldspars, Dass, Bauchi State, NigeriaOyebola Akin-DeluNo ratings yet