You might also like
- Aseptic Technique Lab ReportDocument3 pagesAseptic Technique Lab ReportMarlene Tubieros - Inducil57% (7)
- Clinical Documentation ManualDocument121 pagesClinical Documentation ManualAhmet HadziahmetovicNo ratings yet
- A Systematic Approach To Deep Caries Removal End PointsDocument13 pagesA Systematic Approach To Deep Caries Removal End PointsJosé Misael Aguilar FloresNo ratings yet
- Dha Question BankDocument2 pagesDha Question BankJijo Francis0% (2)
- Dental Plaque - Classification, FormationDocument5 pagesDental Plaque - Classification, FormationRAHMANo ratings yet
- Riccucci Early Enamel LesionsDocument21 pagesRiccucci Early Enamel LesionsМартин АрабаджиевNo ratings yet
- Dental Caries First SessionDocument28 pagesDental Caries First SessionKiana TediNo ratings yet
- CARIOLOGYDocument29 pagesCARIOLOGYjamaica faith ramonNo ratings yet
- Chap 02Document23 pagesChap 02ABNo ratings yet
- Cracked-Tooth Syndrome: Is A Common Result of Incomplete Tooth Fracture. Patients SufferingDocument5 pagesCracked-Tooth Syndrome: Is A Common Result of Incomplete Tooth Fracture. Patients SufferingHayder MaqsadNo ratings yet
- 1 s2.0 S0300571220301767 Main PDFDocument10 pages1 s2.0 S0300571220301767 Main PDFCesar AmaroNo ratings yet
- Management of Deep Carious LesionDocument14 pagesManagement of Deep Carious Lesionahmedstar162000No ratings yet
- Black TriangleDocument6 pagesBlack TriangleAziz IkbalNo ratings yet
- Dentistry 05 00021Document12 pagesDentistry 05 00021anon_628353022No ratings yet
- 10 Dental Caries - 2Document11 pages10 Dental Caries - 2John CenaNo ratings yet
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- Dental CariesDocument5 pagesDental CariesTwinamasiko DanielNo ratings yet
- Dental Wear - A Scanning Electron Microscope Study - 2014Document8 pagesDental Wear - A Scanning Electron Microscope Study - 2014Ana CondeNo ratings yet
- Management of The Deep Carious Lesion A Literature ReviewDocument7 pagesManagement of The Deep Carious Lesion A Literature Reviewمحمد ربيعيNo ratings yet
- Yoshiyama 2002Document5 pagesYoshiyama 2002Eduardo Antonio Mayorga HernandezNo ratings yet
- Etiology and Occurrence of Gingival Recession - An PDFDocument5 pagesEtiology and Occurrence of Gingival Recession - An PDFKurnia FatwatiNo ratings yet
- What Constitutes Dental Caries Histopathology of Carious Enamel and Dentin Related To The Action ofDocument5 pagesWhat Constitutes Dental Caries Histopathology of Carious Enamel and Dentin Related To The Action ofSadeer RiyadNo ratings yet
- Etiology of Periodontal Diseases: Dental Plaque (Microorganisms)Document9 pagesEtiology of Periodontal Diseases: Dental Plaque (Microorganisms)محمد محمود القحيفNo ratings yet
- TALLER 4selwitz2007Document9 pagesTALLER 4selwitz2007Natalia SplashNo ratings yet
- DRJ 19 29Document5 pagesDRJ 19 29janeNo ratings yet
- Biologic Width and Its Relation To PeriodontalDocument7 pagesBiologic Width and Its Relation To PeriodontalBethania CarolinaNo ratings yet
- Dental Caries: Chapter OutlineDocument11 pagesDental Caries: Chapter OutlineairizaNo ratings yet
- Perio Lec.7 Dental Plaque P.1 & P.2Document47 pagesPerio Lec.7 Dental Plaque P.1 & P.2زينNo ratings yet
- Presentation of Histopathology of Dental CariesDocument31 pagesPresentation of Histopathology of Dental CariesShumua ShamiNo ratings yet
- Erupsi Gigi PermanenDocument10 pagesErupsi Gigi PermanenAnggia ParamitaNo ratings yet
- Interpretation of Dental CariesDocument30 pagesInterpretation of Dental Caries202210034No ratings yet
- 4 Pit and FissureDocument74 pages4 Pit and FissureAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Delayed Tooth EmergenceDocument16 pagesDelayed Tooth EmergenceValeria CernegaNo ratings yet
- BelajarDocument9 pagesBelajarmonikaNo ratings yet
- Selective Caries ExcavationDocument10 pagesSelective Caries Excavationjorefe12No ratings yet
- Nihms 798382Document41 pagesNihms 798382Ale MonzalvoNo ratings yet
- 1 s2.0 S106474062100078XDocument8 pages1 s2.0 S106474062100078XTrnrFdy ViveroNo ratings yet
- Tooth Eruption Disorders Associated With Systemic and Genetic Diseases: Clinical GuideDocument16 pagesTooth Eruption Disorders Associated With Systemic and Genetic Diseases: Clinical GuideBanyu علي تقويم BiruNo ratings yet
- Stain 2Document4 pagesStain 2salman khawarNo ratings yet
- Carious Cavities Classification by Black. Features of Carious Cavities Preparation of The 1-st and 5-th Black's ClassesDocument24 pagesCarious Cavities Classification by Black. Features of Carious Cavities Preparation of The 1-st and 5-th Black's ClassesmanarchikNo ratings yet
- Article DentureStomatitis AReviewDocument7 pagesArticle DentureStomatitis AReviewSkAliHassanNo ratings yet
- Dental Hygiene Bab 17Document18 pagesDental Hygiene Bab 17Cinta SalsabilaNo ratings yet
- Eb 79Document5 pagesEb 79mohammad naufalNo ratings yet
- Dental CariesDocument25 pagesDental CariesFemi100% (1)
- UntitledDocument321 pagesUntitledAnalisse PerezNo ratings yet
- 36-1 TunkiwalaDocument16 pages36-1 TunkiwalaSwapnil RastogiNo ratings yet
- Leader, Commission - 1998 - Dental ErosionDocument11 pagesLeader, Commission - 1998 - Dental Erosionjanvier_89No ratings yet
- Time To Shift - From Scaling and Root Planing To Root Surface DebridementDocument5 pagesTime To Shift - From Scaling and Root Planing To Root Surface DebridementYing Yi TeoNo ratings yet
- Dental Caries Andpulpitis20240319Document96 pagesDental Caries Andpulpitis20240319Madhuka SiriwardaneNo ratings yet
- CariesDocument46 pagesCariesginulNo ratings yet
- KB Roopa. J Pediatr DentDocument8 pagesKB Roopa. J Pediatr DentMegha GhoshNo ratings yet
- Oral Prophylaxis: Prophylaxis Remove Dental Plaque and Other IrritantsDocument3 pagesOral Prophylaxis: Prophylaxis Remove Dental Plaque and Other IrritantsjunquelalaNo ratings yet
- Lecture 4 Diagnosis of Dental CariesDocument12 pagesLecture 4 Diagnosis of Dental CariesDt omarNo ratings yet
- Penetration DepthDocument8 pagesPenetration DepthSahasraNo ratings yet
- Occlusal Indicators - A Simplified ApproachDocument8 pagesOcclusal Indicators - A Simplified ApproachDr Tarak ChavadaNo ratings yet
- Chapter 2 DiagnosisDocument24 pagesChapter 2 DiagnosisnilafebryNo ratings yet
- Microbiology of Traumatic InjuryDocument10 pagesMicrobiology of Traumatic InjuryAulia AitaNo ratings yet
- Pit and Fissure SealantsDocument5 pagesPit and Fissure SealantsSimu MedaNo ratings yet
- Ijed 2022 03 s0340CracksGerdolleBrowetDocument17 pagesIjed 2022 03 s0340CracksGerdolleBrowetsousourimeNo ratings yet
- Digital Workflow For The Rehabilitation of The Excessively Worn DentitionDocument26 pagesDigital Workflow For The Rehabilitation of The Excessively Worn Dentitionfloressam2000No ratings yet
- Diagnosis & Pt. AssessmentDocument58 pagesDiagnosis & Pt. Assessmentmahmoud wesamNo ratings yet
- White Spot Lesions: A Literature Review: January 2015Document8 pagesWhite Spot Lesions: A Literature Review: January 2015zulfaNo ratings yet
- Sim PpeDocument16 pagesSim Ppeaurora yangaNo ratings yet
- Europass CV 111004 GalanisDocument2 pagesEuropass CV 111004 GalanisGeorge MastorakisNo ratings yet
- Revised Testing Protocols Inbound and Outbound TravelsDocument5 pagesRevised Testing Protocols Inbound and Outbound Travels64035104No ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaAndri NugrahaNo ratings yet
- Executive Order No 3 Series 2020 Social Amelioration ProgramDocument2 pagesExecutive Order No 3 Series 2020 Social Amelioration ProgramjomarNo ratings yet
- BSA RP Tymp Final 21aug13 FinalDocument20 pagesBSA RP Tymp Final 21aug13 Finalthink positiveNo ratings yet
- Forgein Bodies PPDDocument22 pagesForgein Bodies PPDVishuNo ratings yet
- Pcap FDDocument22 pagesPcap FDJeanne Mae Lee AfallaNo ratings yet
- Infant FeedingDocument7 pagesInfant FeedingAddinFikryNo ratings yet
- Ijerph 18 06796 v2Document24 pagesIjerph 18 06796 v2paolaNo ratings yet
- Pharmacotherapy PlanDocument25 pagesPharmacotherapy PlanMahum SohailNo ratings yet
- Case Write-Up - Beck Institute - Worksheet-Packet - 2020-18-23Document6 pagesCase Write-Up - Beck Institute - Worksheet-Packet - 2020-18-23Carmen-Ioana RotaruNo ratings yet
- Piramal Pharma LimitedDocument3 pagesPiramal Pharma LimitedChandrabali SahaNo ratings yet
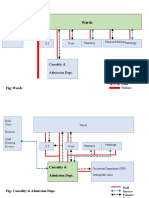
- Wards: Causality & Admission DeptDocument11 pagesWards: Causality & Admission DeptHasib MohammadNo ratings yet
- Colostomy: By: Maria Silvana DhawoDocument15 pagesColostomy: By: Maria Silvana DhawoYohana VetrinelaNo ratings yet
- Asesmen GinekologiDocument15 pagesAsesmen GinekologiYumeko AiharaNo ratings yet
- Dua JameelaDocument14 pagesDua Jameelajannat search of hevenNo ratings yet
- Autoimmune Waterfasting PDFDocument3 pagesAutoimmune Waterfasting PDFMihailo JankovicNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNikko Pananganan DajaoNo ratings yet
- FILARIASISDocument9 pagesFILARIASISAries TiongsonNo ratings yet
- Ignou DatesheetDocument5 pagesIgnou Datesheetsarojit95No ratings yet
- 1-3rd-BDS-Oral Pathology Syllabus 2020Document7 pages1-3rd-BDS-Oral Pathology Syllabus 2020KhanNo ratings yet
- Levels of Evidence Flow Chart Rev May 2019Document3 pagesLevels of Evidence Flow Chart Rev May 2019Karl RobleNo ratings yet
- Walk-In-Interview For Doctors: North Eastern Railway, GorakhpurDocument5 pagesWalk-In-Interview For Doctors: North Eastern Railway, GorakhpurRaghuma Reddy BandaruNo ratings yet
- Minggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusDocument25 pagesMinggu I Miftahul Rauhan Bedah Plastik Ulkus DekubitusmiftahulrauhanNo ratings yet
- Ebp PresentationDocument31 pagesEbp Presentationapi-3148057500% (1)
- Sexually Transmitted Infections (Stis) : 04/15/2022 Haweni A. 1Document57 pagesSexually Transmitted Infections (Stis) : 04/15/2022 Haweni A. 1Cheru DugaseNo ratings yet