You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical Laboratory Science Review by Theriot - JarreauDocument12 pagesClinical Laboratory Science Review by Theriot - JarreauJuneya Koo100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lecture: 2 & 3. Contributions of Pioneeers in The Field of MicrobiologyDocument57 pagesLecture: 2 & 3. Contributions of Pioneeers in The Field of MicrobiologySELVI ANo ratings yet
- कायस्थ समाजके मुल, डेराDocument11 pagesकायस्थ समाजके मुल, डेराdrpklalNo ratings yet
- UG Assessment Form AIIDocument39 pagesUG Assessment Form AIIdrpklalNo ratings yet
- Fap CurriculumDocument8 pagesFap CurriculumdrpklalNo ratings yet
- Teachers Eligibility QualificationsDocument23 pagesTeachers Eligibility QualificationsdrpklalNo ratings yet
- (eHRMS-Electronic Human Resource Management System) : Manav SampadaDocument3 pages(eHRMS-Electronic Human Resource Management System) : Manav SampadadrpklalNo ratings yet
- User Login Manual: National Informatics CentreDocument10 pagesUser Login Manual: National Informatics CentredrpklalNo ratings yet
- Mantra: Embedded Advance AEBAS TerminalDocument3 pagesMantra: Embedded Advance AEBAS TerminaldrpklalNo ratings yet
- Assessment of Quality of Life of HIV-Positive People Receiving ART: An Indian PerspectiveDocument5 pagesAssessment of Quality of Life of HIV-Positive People Receiving ART: An Indian PerspectivedrpklalNo ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- MBBS CURRICULUM 2019 20 Phase 1Document158 pagesMBBS CURRICULUM 2019 20 Phase 1drpklalNo ratings yet
- Assessment of Quality of Life Among Human Immunodeficiency Virus/Acquired Immuno Deficiency Syndrome Patients: A Study at Antiretroviral Therapy Center at Malda, West Bengal, IndiaDocument6 pagesAssessment of Quality of Life Among Human Immunodeficiency Virus/Acquired Immuno Deficiency Syndrome Patients: A Study at Antiretroviral Therapy Center at Malda, West Bengal, IndiadrpklalNo ratings yet
- Mbbs Regulations and Syllabus 2019Document126 pagesMbbs Regulations and Syllabus 2019drpklalNo ratings yet
- Guidelines For Reporting of Figures and Tables For Clinical Research in UrologyDocument13 pagesGuidelines For Reporting of Figures and Tables For Clinical Research in UrologydrpklalNo ratings yet
- Assessment of Quality of Life of HIV-Positive People Receiving ART: An Indian PerspectiveDocument8 pagesAssessment of Quality of Life of HIV-Positive People Receiving ART: An Indian PerspectivedrpklalNo ratings yet
- Quality of Life Among People Living With HIV/AIDS and Its Predictors: A Cross Sectional Study at ART Center, Bagalkot, KarnatakaDocument6 pagesQuality of Life Among People Living With HIV/AIDS and Its Predictors: A Cross Sectional Study at ART Center, Bagalkot, KarnatakadrpklalNo ratings yet
- Factors Influencing Quality of Life Among People Living With HIV in Coastal South IndiaDocument7 pagesFactors Influencing Quality of Life Among People Living With HIV in Coastal South IndiadrpklalNo ratings yet
- Quality of Life Perceptions Amongst Patients Co-Infected With Visceral Leishmaniasis and HIV: A Qualitative Study From Bihar, IndiaDocument14 pagesQuality of Life Perceptions Amongst Patients Co-Infected With Visceral Leishmaniasis and HIV: A Qualitative Study From Bihar, IndiadrpklalNo ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- Quality of Life of People Living With HIV/AIDS Attending Antiretroviral Clinic in The Center of Excellence in HIV Care in IndiaDocument7 pagesQuality of Life of People Living With HIV/AIDS Attending Antiretroviral Clinic in The Center of Excellence in HIV Care in IndiadrpklalNo ratings yet
- Sjams 58e3371 3376Document6 pagesSjams 58e3371 3376drpklalNo ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- Anchala Mahilange - jemds-ORADocument4 pagesAnchala Mahilange - jemds-ORAdrpklalNo ratings yet
- Narasimha Pai Issue 27 Mamatha RathnaDocument7 pagesNarasimha Pai Issue 27 Mamatha RathnadrpklalNo ratings yet
- Prevalence and Antibiotic Susceptibility Pattern of Coagulase Negative Staphylococcus (Cons) in Neonatal SepticemiaDocument4 pagesPrevalence and Antibiotic Susceptibility Pattern of Coagulase Negative Staphylococcus (Cons) in Neonatal SepticemiadrpklalNo ratings yet
- Coagulase Negative Staphylococcus Species : Resistance and Therapeutic Decisions at The Turn of The Novel MillenniumDocument6 pagesCoagulase Negative Staphylococcus Species : Resistance and Therapeutic Decisions at The Turn of The Novel MillenniumdrpklalNo ratings yet
- Speciation and Antibiotic Resistance Pattern of Coagulase Negative Staphylococci (CONS) - Need of TimeDocument8 pagesSpeciation and Antibiotic Resistance Pattern of Coagulase Negative Staphylococci (CONS) - Need of TimedrpklalNo ratings yet
- 286 PDFDocument5 pages286 PDFdrpklalNo ratings yet
- Isolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiaDocument12 pagesIsolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiadrpklalNo ratings yet
- Original Research: Ragini Ananth Kashid, Kausalya RaghuramanDocument5 pagesOriginal Research: Ragini Ananth Kashid, Kausalya RaghuramandrpklalNo ratings yet
- Glauser Et Al (Sept 2019)Document7 pagesGlauser Et Al (Sept 2019)drpklalNo ratings yet
- Velasof PillsbagDocument6 pagesVelasof Pillsbagvijayalakshmi JanakiramanNo ratings yet
- Lab Diagnosis of Diarrheal DiseasesDocument37 pagesLab Diagnosis of Diarrheal DiseasesGIST (Gujarat Institute of Science & Technology)No ratings yet
- Trichuris Trichiura: WhipwormDocument4 pagesTrichuris Trichiura: WhipwormAdhil NirwandiNo ratings yet
- Laboratory Result and InterpretationDocument11 pagesLaboratory Result and Interpretationtzuquino Emz100% (1)
- Family Micrococcaceae and StreptococcaceaeDocument114 pagesFamily Micrococcaceae and StreptococcaceaeAshwani Mathur, Ma-306No ratings yet
- Aspects of Cheetah (Acinonyx Jubatus) Biology, Ecology andDocument516 pagesAspects of Cheetah (Acinonyx Jubatus) Biology, Ecology andZinniaNo ratings yet
- Canine Parvovirus Infection in DogsDocument2 pagesCanine Parvovirus Infection in DogsCharly Lab GumbleNo ratings yet
- (Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Document43 pages(Ped-W1) (Dr. Zuhair M. Al Musawi) Repiratory 2Haider Nadhem AL-rubaiNo ratings yet
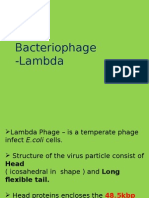
- Lambda PhageDocument21 pagesLambda PhageMagesh RamasamyNo ratings yet
- Icd 10Document1 pageIcd 10renatanurulNo ratings yet
- Cataloguenew 121215100406 Phpapp02Document12 pagesCataloguenew 121215100406 Phpapp02sidomoyoNo ratings yet
- CrisisplanDocument7 pagesCrisisplanapi-299225402No ratings yet
- Are Viruses AliveDocument2 pagesAre Viruses AliveRobert Joseph NikolaiNo ratings yet
- Dentalpharmacology1 130726101143 Phpapp02Document44 pagesDentalpharmacology1 130726101143 Phpapp02Malatesh Sudharshan100% (1)
- Icd 10 Kasus Bedah SarafDocument8 pagesIcd 10 Kasus Bedah SarafHanda YaniNo ratings yet
- Pengendalian Penyakit Terpadu Kanker JerukDocument25 pagesPengendalian Penyakit Terpadu Kanker JerukSelfia rahmiNo ratings yet
- Crab EggsDocument7 pagesCrab EggsNinfa LansangNo ratings yet
- Biodiversity DatabaseDocument11 pagesBiodiversity Databaseakila_easwariNo ratings yet
- Culture MediaDocument6 pagesCulture MediaTryfingNo ratings yet
- FCVDocument23 pagesFCVTrailor BladeNo ratings yet
- HIV & AIDS-WPS OfficeDocument15 pagesHIV & AIDS-WPS OfficeRismaya UlfahNo ratings yet
- Diagnostic Testing For Sars-Cov-2: Interim Guidance 11 September 2020Document20 pagesDiagnostic Testing For Sars-Cov-2: Interim Guidance 11 September 2020Huy Trần ThiệnNo ratings yet
- Measles PathophysiologyDocument1 pageMeasles PathophysiologyAl TheóNo ratings yet
- Enrofloxacin: Therapeutic ReviewDocument4 pagesEnrofloxacin: Therapeutic ReviewAndi Dytha Pramitha SamNo ratings yet
- Acute & Chronic InflammationDocument24 pagesAcute & Chronic Inflammationapi-19916399No ratings yet
- Ebola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisDocument8 pagesEbola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisAuliaZahraNo ratings yet
- Genital WartDocument9 pagesGenital WartJhunel Antonio RomanNo ratings yet
- BabesiaDocument22 pagesBabesiaAbdullah AzeemNo ratings yet