You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hypertension Is Another Name For High Blood PressureDocument91 pagesHypertension Is Another Name For High Blood PressureMd. Sohanul IslamNo ratings yet
- Nbme 18Document49 pagesNbme 18Dilawar Jan95% (38)
- Chapter 9 Active Reading GuideDocument6 pagesChapter 9 Active Reading GuideLâm TặcNo ratings yet
- TIROIDECTOMIIDocument66 pagesTIROIDECTOMIIThoreENo ratings yet
- Basic of ImmunohistochemistryDocument8 pagesBasic of ImmunohistochemistryHanung Puspita Aditya S100% (2)
- Miracle Mineral Supplement - An Integrated TherapyDocument6 pagesMiracle Mineral Supplement - An Integrated TherapyIvan Jankovic100% (1)
- Mrcpi Osce StationsDocument3 pagesMrcpi Osce StationsFA KhanNo ratings yet
- Best Exam Preparation Tips Marlene Pearce PDFDocument32 pagesBest Exam Preparation Tips Marlene Pearce PDFZH. omg sarNo ratings yet
- 3-Curs LMCDocument60 pages3-Curs LMCCristina GheorghiuNo ratings yet
- Finalprintedbook PDFDocument259 pagesFinalprintedbook PDFDejanNo ratings yet
- Guardian Health & Life Insurance FormDocument2 pagesGuardian Health & Life Insurance Formsmbdy tbhhhNo ratings yet
- Expert Systems With Applications: Florin Gorunescu, Smaranda Belciug, Marina Gorunescu, Radu BadeaDocument9 pagesExpert Systems With Applications: Florin Gorunescu, Smaranda Belciug, Marina Gorunescu, Radu BadeaJeena MathewNo ratings yet
- Criteria Donor of BloodDocument3 pagesCriteria Donor of Bloodapi-269388039No ratings yet
- Community Health Survey: Assessment of Resident Health Needs and ConcernsDocument40 pagesCommunity Health Survey: Assessment of Resident Health Needs and ConcernsPreeti SachanNo ratings yet
- AIIMS June 2002 PG Entrance Question Paper With Answer KeyDocument23 pagesAIIMS June 2002 PG Entrance Question Paper With Answer KeywithraviNo ratings yet
- IETADocument10 pagesIETAJose Luis Morales BautistaNo ratings yet
- CA 19-9 11872141001 - enDocument3 pagesCA 19-9 11872141001 - enModestusNo ratings yet
- NIOSH Registry of Toxic Effects of Chemical Substances RTECSDocument186 pagesNIOSH Registry of Toxic Effects of Chemical Substances RTECSNicolás PietrobelliNo ratings yet
- Oral Oncology: SciencedirectDocument7 pagesOral Oncology: SciencedirectafissaNo ratings yet
- UntitledDocument573 pagesUntitledNeil ShebyNo ratings yet
- Medicinal Properties of GarlicDocument7 pagesMedicinal Properties of GarlicFawzia Haznah Nurul Imani0% (1)
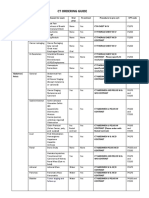
- CT Ordering Guide: Tumor Staging and Follow UpDocument2 pagesCT Ordering Guide: Tumor Staging and Follow UpanonNo ratings yet
- The Benefits of Immunotherapy CombinationsDocument1 pageThe Benefits of Immunotherapy CombinationsMicheleFontanaNo ratings yet
- The Wayland News, August 2009Document20 pagesThe Wayland News, August 2009Julian Horn100% (2)
- Ethnomedicinal Observations Among The Inhabitants of Sarf Naar Area of Shiekhpora Kreeri, Baramulla, Jammu and KashmirDocument4 pagesEthnomedicinal Observations Among The Inhabitants of Sarf Naar Area of Shiekhpora Kreeri, Baramulla, Jammu and KashmirTawseef Ahmad MirNo ratings yet
- Early Life: Seattle Grace Hospital Anatomy JaneDocument2 pagesEarly Life: Seattle Grace Hospital Anatomy JaneGit GitaNo ratings yet
- Pet CT ReviewDocument5 pagesPet CT ReviewKotarou BokutoNo ratings yet
- Gastro-Oesophageal Reflux Disease: EpidemiologyDocument6 pagesGastro-Oesophageal Reflux Disease: EpidemiologyRehan RiyazNo ratings yet
- Incontinencia Urinaria Fisiopatologia The Clinics PDFDocument12 pagesIncontinencia Urinaria Fisiopatologia The Clinics PDFOmar Teran LinaresNo ratings yet
- Melasma 56 Pacientes CoreanosDocument10 pagesMelasma 56 Pacientes CoreanosSuzana PoloncaNo ratings yet