You might also like
- The Late Talker: What to Do If Your Child Isn't Talking YetFrom EverandThe Late Talker: What to Do If Your Child Isn't Talking YetRating: 4 out of 5 stars4/5 (4)
- Teach Reading with Orton-Gillingham: 72 Classroom-Ready Lessons to Help Struggling Readers and Students with Dyslexia Learn to Love ReadingFrom EverandTeach Reading with Orton-Gillingham: 72 Classroom-Ready Lessons to Help Struggling Readers and Students with Dyslexia Learn to Love ReadingRating: 5 out of 5 stars5/5 (1)
- Learning Disabilities and School Failure - Ped Rev Aug 2011Document12 pagesLearning Disabilities and School Failure - Ped Rev Aug 2011diaspalma.medNo ratings yet
- Learning Disability and Behaviour Problems Among School Going ChildrenDocument6 pagesLearning Disability and Behaviour Problems Among School Going ChildrenDishuNo ratings yet
- Early Developmental Delays - A Cross Validation StudyDocument5 pagesEarly Developmental Delays - A Cross Validation StudyfadhlialbaniNo ratings yet
- Specific Learning DisorderDocument7 pagesSpecific Learning Disordersunainanajeeb777No ratings yet
- Evaluation of Children With Reading DifficultiesDocument8 pagesEvaluation of Children With Reading Difficultiesandreiagome4444No ratings yet
- Rimrodt, S. L., & Lipkin, P. H. (2011) Learning Disabilities and School Failure Pediatrics in ReviewDocument12 pagesRimrodt, S. L., & Lipkin, P. H. (2011) Learning Disabilities and School Failure Pediatrics in ReviewSdNNo ratings yet
- Language Development and Its Impact On Childrens Psychosocial and Emotional DevelopmentDocument6 pagesLanguage Development and Its Impact On Childrens Psychosocial and Emotional DevelopmentTatiana Mina CambindoNo ratings yet
- Reading challenges and coping strategies of junior high studentsDocument14 pagesReading challenges and coping strategies of junior high studentsjonalyn obinaNo ratings yet
- Prevalence of Dyslexia Among Children Aged 7 To 9 in Nairobi, KenyaDocument44 pagesPrevalence of Dyslexia Among Children Aged 7 To 9 in Nairobi, Kenyaismail39 orthoNo ratings yet
- RD - Mental Health in Deaf Children (Data Kesehatan Mental Tunarungu)Document2 pagesRD - Mental Health in Deaf Children (Data Kesehatan Mental Tunarungu)dennyabdurrachman20No ratings yet
- EarlyDocument12 pagesEarlyCostiNo ratings yet
- Early Identification and Interventions For Dyslexia: A Contemporary ViewDocument9 pagesEarly Identification and Interventions For Dyslexia: A Contemporary Viewapi-313799104No ratings yet
- Early Intervention For ReadingDocument1 pageEarly Intervention For ReadingLinda Balsiger100% (1)
- Down Syndrome School Entry SkillsDocument7 pagesDown Syndrome School Entry SkillsKimmy ChuNo ratings yet
- Accelerating research on emotional and behavioral problems in learning disabilitiesDocument10 pagesAccelerating research on emotional and behavioral problems in learning disabilitiesGeorgiana CretuNo ratings yet
- Down Syndrome Students: Mainstream vs Special EducationDocument12 pagesDown Syndrome Students: Mainstream vs Special EducationHanny ReyesNo ratings yet
- Northland Community and Technical College Occupational Therapy Assistant Program Critically Appraised Topics Assignment Bailly SagerDocument12 pagesNorthland Community and Technical College Occupational Therapy Assistant Program Critically Appraised Topics Assignment Bailly Sagerapi-285542134No ratings yet
- Action Research Paper FinalDocument24 pagesAction Research Paper Finalapi-473349564No ratings yet
- Acrefore 9780199975839 e 1218Document16 pagesAcrefore 9780199975839 e 1218Francisca PuriceNo ratings yet
- Ebd12r PDFDocument8 pagesEbd12r PDFVera Dyah SaputriNo ratings yet
- Case Study AnalysisDocument16 pagesCase Study AnalysisDan PaulNo ratings yet
- Science 2009 GabrielDocument5 pagesScience 2009 GabrielMago Hugo HugoNo ratings yet
- Primary Prevention Knowledge of Parents and Teachers of Nursery and Play Group On Childhood Sexual AbuseDocument6 pagesPrimary Prevention Knowledge of Parents and Teachers of Nursery and Play Group On Childhood Sexual AbuseMuhammad Malik HakimNo ratings yet
- Review Article: Psychological Co Morbidity in Children and Adolescents With Learning DisordersDocument5 pagesReview Article: Psychological Co Morbidity in Children and Adolescents With Learning DisordersHayati Rizki PutriNo ratings yet
- Action ResearchDocument11 pagesAction ResearchMaribel Cabaya Soliven0% (1)
- Early Warning System: by G. Reid Lyon & Jack M. FletcherDocument9 pagesEarly Warning System: by G. Reid Lyon & Jack M. FletcherGauravKrishnaNo ratings yet
- Concept2 DanlagDocument4 pagesConcept2 DanlagLouweben MaquizoNo ratings yet
- King Dowling2015Document8 pagesKing Dowling2015lis rocioNo ratings yet
- Interpersonal Behavioural Problems in Children With Hearing Impairment: The Parental Experiences and Coping StrategiesDocument14 pagesInterpersonal Behavioural Problems in Children With Hearing Impairment: The Parental Experiences and Coping StrategiesKhaedirul FaqihNo ratings yet
- The Influence of Family Factors On Children Early Literacy SkillsDocument28 pagesThe Influence of Family Factors On Children Early Literacy SkillsSalman HasibuanNo ratings yet
- PediatricsPaper 9-16-2019 Plaintext PreprintDocument22 pagesPediatricsPaper 9-16-2019 Plaintext PreprintMălina CorlătianuNo ratings yet
- Jurnal Reading Speech and Language IKA FIXDocument20 pagesJurnal Reading Speech and Language IKA FIXNadyklaNo ratings yet
- LIDO - Mclntyre 2017 - Reading ProfilesDocument16 pagesLIDO - Mclntyre 2017 - Reading ProfilesDébora PiazarolloNo ratings yet
- 192060-Article Text-487046-1-10-20200107eeeDocument17 pages192060-Article Text-487046-1-10-20200107eeeAlex JuravleNo ratings yet
- Pred ProjectDocument19 pagesPred ProjectYeliz YılmazNo ratings yet
- 1st SourceDocument10 pages1st Sourceapi-581791742No ratings yet
- Identification Guide for Children with Specific Learning DisabilitiesDocument9 pagesIdentification Guide for Children with Specific Learning DisabilitiesS3 ILMU PENDIDIKANNo ratings yet
- DraftoutlineDocument21 pagesDraftoutlineapi-273272895No ratings yet
- Early Human DevelopmentDocument7 pagesEarly Human DevelopmentAndrés GordilloNo ratings yet
- Pediatrics 2013Document9 pagesPediatrics 2013Bella AgiusselaNo ratings yet
- Dialogic Reading for Child Language Growth in South AfricaDocument11 pagesDialogic Reading for Child Language Growth in South AfricaJardín FlorestaNo ratings yet
- Specific Learning DisorderDocument27 pagesSpecific Learning DisorderJovencio MarquezNo ratings yet
- Improving life skills in children with Down SyndromeDocument3 pagesImproving life skills in children with Down SyndromeNehla FirozNo ratings yet
- ContentServer Monica2Document23 pagesContentServer Monica2Luis.fernando. GarciaNo ratings yet
- Hulme 2016Document5 pagesHulme 2016raraNo ratings yet
- LD-Practice Guidelines - India 2011 PDFDocument48 pagesLD-Practice Guidelines - India 2011 PDFnesumaNo ratings yet
- Challenges Related To Educational Interpreting For Students Who Are Deaf With DisabilitiesDocument12 pagesChallenges Related To Educational Interpreting For Students Who Are Deaf With DisabilitiesVictor Rivera100% (1)
- Center-Based Child Care and Differential Improvements in The Child Development Outcomes of Disadvantaged ChildrenDocument26 pagesCenter-Based Child Care and Differential Improvements in The Child Development Outcomes of Disadvantaged ChildrenmanckadalNo ratings yet
- Boosting Kindergarten Reading Skills with Targeted InterventionDocument56 pagesBoosting Kindergarten Reading Skills with Targeted Interventionshazura_75No ratings yet
- Pervasive Developmental Disorder Not Otherwise SpecifiedDocument7 pagesPervasive Developmental Disorder Not Otherwise SpecifiedAlexander DeckerNo ratings yet
- European Journal of Pediatrics SciDocument7 pagesEuropean Journal of Pediatrics ScianimeshNo ratings yet
- Reading Difficulties and Attention-Deficit/ Hyperactivity Behaviours: Evidence of An Early Association in A Nonclinical SampleDocument18 pagesReading Difficulties and Attention-Deficit/ Hyperactivity Behaviours: Evidence of An Early Association in A Nonclinical SampleNani JuraidaNo ratings yet
- Effects of Hearing Loss On Academic Performance On Pupils With Hearing Loss.Document6 pagesEffects of Hearing Loss On Academic Performance On Pupils With Hearing Loss.appiah ernestNo ratings yet
- Identifying Children at Risk For Language Impairment or Dyslexia With Group-Administered MeasuresDocument16 pagesIdentifying Children at Risk For Language Impairment or Dyslexia With Group-Administered MeasuresAfif RahmanNo ratings yet
- Dyslexic Children: The Need For Parents AwarenessDocument9 pagesDyslexic Children: The Need For Parents AwarenessJoi JenozNo ratings yet
- And Children's Internalizing, Externalizing Behavior Problems and Academic AchievementDocument8 pagesAnd Children's Internalizing, Externalizing Behavior Problems and Academic AchievementTuấn KhangNo ratings yet
- Behavioural, Emotional and Social Development of Children Who StutterDocument10 pagesBehavioural, Emotional and Social Development of Children Who StutterMagaliNo ratings yet
- Trajectories-of-prosociality-from-early-to-middle-chil_2020_Journal-of-CommuDocument11 pagesTrajectories-of-prosociality-from-early-to-middle-chil_2020_Journal-of-CommuRaya StefanovaNo ratings yet
- Maps of India - PDF KASARGODEDocument3 pagesMaps of India - PDF KASARGODEsubhashkpn86No ratings yet
- Daily tasks enslave without clear goalsDocument1 pageDaily tasks enslave without clear goalssubhashkpn86No ratings yet
- Star-Delta TransformationDocument7 pagesStar-Delta TransformationAbhijit Kar Gupta80% (5)
- Innovative Solution: Hesop: Mr. Swarup ChakrabortyDocument13 pagesInnovative Solution: Hesop: Mr. Swarup Chakrabortysubhashkpn86No ratings yet
- 1001 Books You Must Read Before You Die - The Definitive ListDocument120 pages1001 Books You Must Read Before You Die - The Definitive ListCraig Smith33% (3)
- Abb Ref615-2Document186 pagesAbb Ref615-2frajaprNo ratings yet
- Earthing (Grounding) and Bonding Guidelines For Uniprise Solutions F/UTP Cabling SystemDocument11 pagesEarthing (Grounding) and Bonding Guidelines For Uniprise Solutions F/UTP Cabling Systemcharleselitb92No ratings yet
- Ovpd VoltageDocument3 pagesOvpd Voltagesubhashkpn86No ratings yet
- 191792Document3 pages191792subhashkpn86No ratings yet
- TPC Monthly Checklist For July 2016Document3 pagesTPC Monthly Checklist For July 2016subhashkpn86No ratings yet
- MB Manual Ga-H110m-S2 (Ddr3) eDocument38 pagesMB Manual Ga-H110m-S2 (Ddr3) esubhashkpn86No ratings yet
- Brochure Rectifier Sg825863ben c00!09!2016 LRDocument8 pagesBrochure Rectifier Sg825863ben c00!09!2016 LRsubhashkpn86No ratings yet
- Attendance - Jul 16Document5 pagesAttendance - Jul 16subhashkpn86No ratings yet
- Learning Disabilities in Children: Epidemiology, Risk Factors and Importance of Early InterventionDocument7 pagesLearning Disabilities in Children: Epidemiology, Risk Factors and Importance of Early Interventionsubhashkpn86No ratings yet
- Earth Rods Fitness Check RecordDocument2 pagesEarth Rods Fitness Check Recordsubhashkpn86No ratings yet
- Monthly traction power consumption reportDocument5 pagesMonthly traction power consumption reportsubhashkpn86No ratings yet
- Tendering Process CVC GuidelinesDocument26 pagesTendering Process CVC GuidelinesshriramNo ratings yet
- NightDocument1 pageNightsubhashkpn86No ratings yet
- Book 1Document18 pagesBook 1subhashkpn86No ratings yet
- QHE - DAC - 001 List of DocumentsDocument263 pagesQHE - DAC - 001 List of Documentssubhashkpn86No ratings yet
- TPC Monthly ChecklistDocument3 pagesTPC Monthly Checklistsubhashkpn86No ratings yet
- Telangana Weather Forecast Heavy Rain LikelyDocument1 pageTelangana Weather Forecast Heavy Rain Likelysubhashkpn86No ratings yet
- SPN Book DetailsDocument10 pagesSPN Book Detailssubhashkpn86No ratings yet
- WF 25072016Document1 pageWF 25072016subhashkpn86No ratings yet
- Telangana Weather Forecast Heavy Rain LikelyDocument1 pageTelangana Weather Forecast Heavy Rain Likelysubhashkpn86No ratings yet
- HRE - WTS - 001 - Weekly Training Schedule (July To Aug)Document56 pagesHRE - WTS - 001 - Weekly Training Schedule (July To Aug)subhashkpn86No ratings yet
- PTW Execution RecordDocument32 pagesPTW Execution Recordsubhashkpn86No ratings yet
- AnsiDocument1 pageAnsihm_4sNo ratings yet
- WF 25072016Document1 pageWF 25072016subhashkpn86No ratings yet
- Introduction MdaDocument5 pagesIntroduction MdaRahasti HerliapsariNo ratings yet
- F20 WorksheetDocument6 pagesF20 WorksheetAbdul HannanNo ratings yet
- Jyotish - Marc Boney - Babel's Tower - The Astrology of PolyglotsDocument42 pagesJyotish - Marc Boney - Babel's Tower - The Astrology of PolyglotsRajesh S VNo ratings yet
- Status ControlDocument62 pagesStatus ControlnormuchNo ratings yet
- 3zr ToyotaDocument9 pages3zr ToyotaDavid ParariNo ratings yet
- Pastoral TheologyDocument4 pagesPastoral TheologyIlli KrineisNo ratings yet
- REIKIREIDOmanual PDFDocument3 pagesREIKIREIDOmanual PDFIancu AdrianNo ratings yet
- 2023 2 FINAL EXAM LEVEL V UNITS 9 & 10 TOPNOTCH 2B 50 QsDocument4 pages2023 2 FINAL EXAM LEVEL V UNITS 9 & 10 TOPNOTCH 2B 50 Qsenelitajorgito.1991No ratings yet
- Eminem - Kill You Lyrics - Genius LyricsDocument18 pagesEminem - Kill You Lyrics - Genius LyricsMarc Roca BOscNo ratings yet
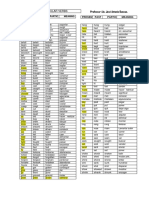
- Irregular Verbs Nueva Lista DuncanDocument2 pagesIrregular Verbs Nueva Lista DuncanAndrey Vargas MoralesNo ratings yet
- Singing is good for your soul! Top tips for voice careDocument1 pageSinging is good for your soul! Top tips for voice carePeter DerrickNo ratings yet
- Two Irrational Numbers Whose Sum Is RationalDocument4 pagesTwo Irrational Numbers Whose Sum Is RationalnishagoyalNo ratings yet
- Dli 8Document174 pagesDli 8Măriuca MăryNo ratings yet
- ESP Course and Syllabus Design Paper PDFDocument23 pagesESP Course and Syllabus Design Paper PDFputri novaNo ratings yet
- Access Gr7 PDFDocument168 pagesAccess Gr7 PDFSprinter Transit Van0% (1)
- Usage of AUTOSAR Diagnostic Modules in A MOST Electronic Control UnitDocument4 pagesUsage of AUTOSAR Diagnostic Modules in A MOST Electronic Control UnitAnubhav JainNo ratings yet
- English Test 5thDocument3 pagesEnglish Test 5thAnny MonsalveNo ratings yet
- Analysis of Moral Values in Jojo Rabbit MovieDocument13 pagesAnalysis of Moral Values in Jojo Rabbit MovieJade Leonor Báez MedinaNo ratings yet
- Week 5 Le Eng 10 Quarter 1Document4 pagesWeek 5 Le Eng 10 Quarter 1Neneth BalsamoNo ratings yet
- Kindergarten Homework FolderDocument7 pagesKindergarten Homework FolderMaria ReyesNo ratings yet
- Cache Memory: Maninder KaurDocument18 pagesCache Memory: Maninder KaurMisha AnonyNo ratings yet
- What Does A Statistical Test DoDocument16 pagesWhat Does A Statistical Test DoRenato PanesNo ratings yet
- Pembahasan Soal Day 4Document6 pagesPembahasan Soal Day 4adeliazabrinaNo ratings yet
- Buri NazarDocument2 pagesBuri NazarS1536097F0% (1)
- TranscriptDocument2 pagesTranscriptapi-379818799No ratings yet
- Next Generation Network Addressing SolutionsDocument318 pagesNext Generation Network Addressing SolutionspvsairamNo ratings yet
- Oracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFDocument258 pagesOracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFKuldeep Singh50% (2)
- 1.manual 1.1 Lite ENG Rev12 19Document11 pages1.manual 1.1 Lite ENG Rev12 19Ding Ching TingNo ratings yet
- The Global Presence of The Ancient Indigenous Moors VolumesDocument2 pagesThe Global Presence of The Ancient Indigenous Moors Volumesev3ldash100% (1)
- Book VI: Yuddha Kanda - Book of WarDocument6 pagesBook VI: Yuddha Kanda - Book of WarGerald PennNo ratings yet