You might also like
- Models of Protection Against HIV/SIV: Models of Protection Against HIV/SIVFrom EverandModels of Protection Against HIV/SIV: Models of Protection Against HIV/SIVGianfranco PancinoNo ratings yet
- Review: Lucia Romani, Andrew C Steer, Margot J Whitfeld, John M KaldorDocument8 pagesReview: Lucia Romani, Andrew C Steer, Margot J Whitfeld, John M KaldorMuhammad AmrullahNo ratings yet
- Prevalence of Scabies and Impetigo Worldwide: A Systematic ReviewDocument9 pagesPrevalence of Scabies and Impetigo Worldwide: A Systematic ReviewNgennest HimNo ratings yet
- Covid-19 Infection and PregnancyFrom EverandCovid-19 Infection and PregnancyAhmed M. Maged El-GolyNo ratings yet
- Scabies: Application of The Novel Identify-Isolate-Inform Tool For Detection and ManagementDocument8 pagesScabies: Application of The Novel Identify-Isolate-Inform Tool For Detection and Managementraudhatul muttaqinNo ratings yet
- Scabies Application of The No PDFDocument10 pagesScabies Application of The No PDFYosia KevinNo ratings yet
- Infectious SpondylodiscitisDocument12 pagesInfectious SpondylodiscitisRoxana StanciuNo ratings yet
- The Global Burden of Scabies: A Cross-Sectional Analysis From The Global Burden of Disease Study 2015Document12 pagesThe Global Burden of Scabies: A Cross-Sectional Analysis From The Global Burden of Disease Study 2015Ade Lia PebrianiNo ratings yet
- Diagnostics For COVID-19Document12 pagesDiagnostics For COVID-19JOHN WALSHNo ratings yet
- The Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisDocument10 pagesThe Cascade of Care in Diagnosis and Treatment of Latent Tuberculosis Infection: A Systematic Review and Meta-AnalysisArdi_xNo ratings yet
- Accepted Manuscript: Acta TropicaDocument24 pagesAccepted Manuscript: Acta TropicaakshayajainaNo ratings yet
- Scabies Outbreaks in Ten Care Homes For Elderly People: A Prospective Study of Clinical Features, Epidemiology, and Treatment OutcomesDocument9 pagesScabies Outbreaks in Ten Care Homes For Elderly People: A Prospective Study of Clinical Features, Epidemiology, and Treatment OutcomesyoggihermawanNo ratings yet
- Definisi Klasifikasi Etiologi Dan ManifeDocument11 pagesDefinisi Klasifikasi Etiologi Dan ManifenatassyamarizNo ratings yet
- The Public Health Control of SDocument13 pagesThe Public Health Control of SYosia KevinNo ratings yet
- Jurnal Ing MK 4Document10 pagesJurnal Ing MK 4Iffah AlhikmahNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- IDSA Guias Infeccion de Tejidos Blandos 2014 PDFDocument43 pagesIDSA Guias Infeccion de Tejidos Blandos 2014 PDFyonaNo ratings yet
- Lancet Infect Dis 2016 - Zoonotic TB (4172)Document5 pagesLancet Infect Dis 2016 - Zoonotic TB (4172)Shahzeen Sajid KhanNo ratings yet
- The Potential For A Blood Test For Scabies: BackgroundDocument12 pagesThe Potential For A Blood Test For Scabies: BackgroundMaya QadrianiNo ratings yet
- Trop Med 140515Document10 pagesTrop Med 140515Arfa AlyaNo ratings yet
- Running Head: Health Impact Framework/Research Paper 1Document10 pagesRunning Head: Health Impact Framework/Research Paper 1api-395030165No ratings yet
- Mycobacterium Tuberculosis DissertationDocument8 pagesMycobacterium Tuberculosis DissertationDoMyPaperForMeSingapore100% (1)
- The Global Distribution of The Arbovirus Vectors Aedes Aegypti and Ae. AlbopictusDocument18 pagesThe Global Distribution of The Arbovirus Vectors Aedes Aegypti and Ae. AlbopictusRenaldi ArdiyaNo ratings yet
- An Approach For Corona Spreads Forecast and Herd Immunity Prediction With The Help of Machine LearningDocument12 pagesAn Approach For Corona Spreads Forecast and Herd Immunity Prediction With The Help of Machine LearningAmina ShaikhNo ratings yet
- Communicable Disease Surveillance: OfepidemiologyDocument4 pagesCommunicable Disease Surveillance: OfepidemiologyMuhammad Hafiidh MuizzNo ratings yet
- Journal PNTD 0009577Document17 pagesJournal PNTD 0009577Khusnul Catur PutriNo ratings yet
- Prospective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiesDocument17 pagesProspective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiespunyayaNo ratings yet
- Impetigo SurveilensDocument10 pagesImpetigo SurveilensSitipradyta KasimNo ratings yet
- Monkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Document14 pagesMonkeypox Virus Infection in Humans Across 16 Countries - April-June 2022Raphael Chalbaud Biscaia HartmannNo ratings yet
- Scabies PRDocument6 pagesScabies PRAnnisa KartikasariNo ratings yet
- Transmission Routes of Rare Seasonal Diseases - The Case of Norovirus InfectionsDocument8 pagesTransmission Routes of Rare Seasonal Diseases - The Case of Norovirus InfectionsPeteNo ratings yet
- Daily Use of Lateral Flow Devices by Contacts of CDocument12 pagesDaily Use of Lateral Flow Devices by Contacts of CCláudia SilvaNo ratings yet
- Clin Infect Dis. 2014 Stevens Cid - Ciu296Document43 pagesClin Infect Dis. 2014 Stevens Cid - Ciu296Kiran SurageNo ratings yet
- CDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexDocument16 pagesCDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexkikiNo ratings yet
- Understanding Risk Communication For Prevention and Control of Vector-Borne Diseases: A Mixed-Method Study in Curac AoDocument22 pagesUnderstanding Risk Communication For Prevention and Control of Vector-Borne Diseases: A Mixed-Method Study in Curac AoAbel Abelito Jimenez Jimenez Jr.No ratings yet
- J of Small Animal Practice - 2020 - Wallis - A Review of The Frequency and Impact of Periodontal Disease in DogsDocument12 pagesJ of Small Animal Practice - 2020 - Wallis - A Review of The Frequency and Impact of Periodontal Disease in Dogskrystell.aguilar95No ratings yet
- Sti GuidelinesDocument43 pagesSti GuidelinesagusNo ratings yet
- Civ 028Document9 pagesCiv 028Deah RisbaNo ratings yet
- Lessons From The Response To The Threat of Transfusion Transmitted VCJD in Ireland 2013 Transfusion Clinique Et BiologiqueDocument6 pagesLessons From The Response To The Threat of Transfusion Transmitted VCJD in Ireland 2013 Transfusion Clinique Et BiologiqueahlemNo ratings yet
- Global Health Current Issues Future Trends and ForDocument8 pagesGlobal Health Current Issues Future Trends and ForMsMhey PalattaoNo ratings yet
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNo ratings yet
- Scabies Lapsus 4Document18 pagesScabies Lapsus 4gabbynengNo ratings yet
- The Diagnosis of Scabies by Non-Expert Examiners: A Study of Diagnostic AccuracyDocument13 pagesThe Diagnosis of Scabies by Non-Expert Examiners: A Study of Diagnostic AccuracyAnisa Rifkia ZSNo ratings yet
- Jvetres 62 027 PDFDocument8 pagesJvetres 62 027 PDFCintia FloresNo ratings yet
- Telehealth For Global Emergencies: Implications For Coronavirus Disease 2019 (COVID-19)Document6 pagesTelehealth For Global Emergencies: Implications For Coronavirus Disease 2019 (COVID-19)Niki Pratiwi WijayaNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General Reviewsuryanto_malvinNo ratings yet
- Scabies Mites Alter The Skin Microbiome and PromoteDocument13 pagesScabies Mites Alter The Skin Microbiome and Promotemohammed bouchibaNo ratings yet
- A Case Report of Crusted ScabiesDocument7 pagesA Case Report of Crusted ScabiesKlinik Pratama Ar-Raudhah 129No ratings yet
- CelullitisDocument43 pagesCelullitisann_1983No ratings yet
- Practice Guidelines For The Diagnosis IDSA 2014 Infecã Ã o de Partes MolesDocument43 pagesPractice Guidelines For The Diagnosis IDSA 2014 Infecã Ã o de Partes MolesRafael SuzukiNo ratings yet
- Newly Identified Viruses in Human Gastroenteritis: Espid R RDocument4 pagesNewly Identified Viruses in Human Gastroenteritis: Espid R RArianne LasamNo ratings yet
- Dengue Virus DissertationDocument7 pagesDengue Virus DissertationDoMyCollegePaperJackson100% (1)
- Burgunder2022 Article MedicationAndFluidManagementOfDocument13 pagesBurgunder2022 Article MedicationAndFluidManagementOfNaomy Castan IbarraNo ratings yet
- Current Pathogens Infecting Open Fracture Tibia and Their Antibiotic Susceptibility at A Tertiary Care Teaching Hospital in South East AsiaDocument10 pagesCurrent Pathogens Infecting Open Fracture Tibia and Their Antibiotic Susceptibility at A Tertiary Care Teaching Hospital in South East AsiaFrancis RomanosNo ratings yet
- Multisystem Inflammatory Syndrome in Children A Systematic ReviewDocument16 pagesMultisystem Inflammatory Syndrome in Children A Systematic ReviewAnna De AguasNo ratings yet
- 1 McCaffrey - Global CementDocument26 pages1 McCaffrey - Global CementJohnNo ratings yet
- Medi 97 E11097Document4 pagesMedi 97 E11097Lia FikayuniarNo ratings yet
- Vaccines For COVID-19 The Current State of PlayDocument8 pagesVaccines For COVID-19 The Current State of PlayNazmul IslamNo ratings yet
- Civ 609Document17 pagesCiv 609Descargar scribdNo ratings yet
- Definition of Metropolitan Region in Various Countries: Definition by DickinsonDocument3 pagesDefinition of Metropolitan Region in Various Countries: Definition by Dickinsonaditi kaviwalaNo ratings yet
- (Psychology of Learning and Motivation 60) Brian H. Ross (Eds.) - Psychology of Learning and Motivation, Volume 60-Academic Press (2014)Document361 pages(Psychology of Learning and Motivation 60) Brian H. Ross (Eds.) - Psychology of Learning and Motivation, Volume 60-Academic Press (2014)AutosmartNo ratings yet
- 10 1016@j Copsyc 2020 04 005Document6 pages10 1016@j Copsyc 2020 04 005terminallllNo ratings yet
- Assignment Brief Unit 47 QCFDocument14 pagesAssignment Brief Unit 47 QCFAlamzeb KhanNo ratings yet
- Chapter - 3 Rev 2Document11 pagesChapter - 3 Rev 2Merin sunilNo ratings yet
- Syllabus HE20203Document2 pagesSyllabus HE20203Pua Suan Jin RobinNo ratings yet
- Contribution of Tourism Industry in Indian Economy: An AnalysisDocument8 pagesContribution of Tourism Industry in Indian Economy: An AnalysisHarsh GuptaNo ratings yet
- Midterm Fall 2019Document8 pagesMidterm Fall 2019NEERAJ KUMARNo ratings yet
- Assessment Techniques of Affective DomainDocument32 pagesAssessment Techniques of Affective DomainSanthosh.S.UNo ratings yet
- Introduction To Nursing ResearchDocument17 pagesIntroduction To Nursing ResearchYounas BhattiNo ratings yet
- NBS Special Publication 260-100Document104 pagesNBS Special Publication 260-100Mauricio arteaga salinasNo ratings yet
- Application Prototype Test and Design ReportDocument6 pagesApplication Prototype Test and Design ReportAndreea-Daniela EneNo ratings yet
- Instructional Supervisory Plan Cajidiocan CES 2022Document8 pagesInstructional Supervisory Plan Cajidiocan CES 2022Mariel Romero100% (1)
- Badoi A. 387318 PDFDocument53 pagesBadoi A. 387318 PDFIrna P LestariNo ratings yet
- A Study On Training & Development in Kurnool: Yamaha Motors P.Chakrapani ReddyDocument7 pagesA Study On Training & Development in Kurnool: Yamaha Motors P.Chakrapani ReddybagyaNo ratings yet
- S1 Ciceral, A. (1982) Interviews, Surveys and The Problem of Ecological Validity PDFDocument11 pagesS1 Ciceral, A. (1982) Interviews, Surveys and The Problem of Ecological Validity PDFmppudp100% (1)
- Change Your Business With NLP: Powerful Tools To Improve Your Organisation's Performance and Get ResultsDocument28 pagesChange Your Business With NLP: Powerful Tools To Improve Your Organisation's Performance and Get ResultsCapstone Publishing100% (3)
- SCM201 - Ôn Quiz 2Document38 pagesSCM201 - Ôn Quiz 2Quỳnh Lê DiễmNo ratings yet
- CORE 1 - Assess Market OpportunitiesDocument76 pagesCORE 1 - Assess Market OpportunitiesMarizon Pagalilauan Muñiz100% (4)
- World Inbox 1 Mock TestDocument26 pagesWorld Inbox 1 Mock TestVidhnesh SoniNo ratings yet
- 4.+Jurnal+TC+Desember+2021 Fix-63-78 CompressedDocument16 pages4.+Jurnal+TC+Desember+2021 Fix-63-78 CompressedRahayu Syahdila FitriNo ratings yet
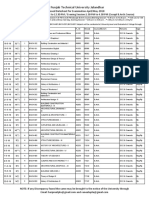
- Prposed Date Sheet Upload Web SiteDocument154 pagesPrposed Date Sheet Upload Web SiteShaheer ShafatNo ratings yet
- Lazarus Final Report 2011Document7 pagesLazarus Final Report 2011ratzzuscaNo ratings yet
- Tax Research MemoDocument2 pagesTax Research MemoSeth9362767720% (1)
- ALMANYA CHAWLA Finale ReportDocument60 pagesALMANYA CHAWLA Finale ReportAseemNo ratings yet
- Contingency Theory - "Complex Man" or "Complex Organization"? PDFDocument16 pagesContingency Theory - "Complex Man" or "Complex Organization"? PDFlucasNo ratings yet
- HR Planning ArticleDocument17 pagesHR Planning Articlegagan_9989495No ratings yet
- 1 - Chapter 1 of Your Textbook Describes The Purposes of Nursing ResearDocument4 pages1 - Chapter 1 of Your Textbook Describes The Purposes of Nursing ResearHelping TutorsNo ratings yet
- G10 Research Paper Student Guide BookletDocument15 pagesG10 Research Paper Student Guide BookletNara BrNo ratings yet
- Factors Affecting Brand Loyalty in Smart Phone Industry: Presented by Soma ArjunDocument18 pagesFactors Affecting Brand Loyalty in Smart Phone Industry: Presented by Soma ArjunThiru ArunNo ratings yet
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessFrom EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNo ratings yet
- Merle's Door: Lessons from a Freethinking DogFrom EverandMerle's Door: Lessons from a Freethinking DogRating: 4 out of 5 stars4/5 (326)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueFrom EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueRating: 4.5 out of 5 stars4.5/5 (31)
- The Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationFrom EverandThe Dog Listener: Learn How to Communicate with Your Dog for Willing CooperationRating: 4 out of 5 stars4/5 (37)
- Roxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueFrom EverandRoxane Gay & Everand Originals Presents: Good Girl: Notes on Dog RescueRating: 5 out of 5 stars5/5 (4)
- Will's Red Coat: The Story of One Old Dog Who Chose to Live AgainFrom EverandWill's Red Coat: The Story of One Old Dog Who Chose to Live AgainRating: 4.5 out of 5 stars4.5/5 (18)
- Lucky Dog Lessons: Train Your Dog in 7 DaysFrom EverandLucky Dog Lessons: Train Your Dog in 7 DaysRating: 4.5 out of 5 stars4.5/5 (41)
- Show Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredFrom EverandShow Dog: The Charmed Life and Trying Times of a Near-Perfect PurebredRating: 3.5 out of 5 stars3.5/5 (13)
- The Other End of the Leash: Why We Do What We Do Around DogsFrom EverandThe Other End of the Leash: Why We Do What We Do Around DogsRating: 5 out of 5 stars5/5 (65)
- An Eagle Named Freedom: My True Story of a Remarkable FriendshipFrom EverandAn Eagle Named Freedom: My True Story of a Remarkable FriendshipNo ratings yet
- The Stress Factor in Dogs: Unlocking Resiliency and Enhancing Well-BeingFrom EverandThe Stress Factor in Dogs: Unlocking Resiliency and Enhancing Well-BeingRating: 5 out of 5 stars5/5 (1)
- Dogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowFrom EverandDogland: Passion, Glory, and Lots of Slobber at the Westminster Dog ShowNo ratings yet
- Come Back, Como: Winning the Heart of a Reluctant DogFrom EverandCome Back, Como: Winning the Heart of a Reluctant DogRating: 3.5 out of 5 stars3.5/5 (10)
- The Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsFrom EverandThe Dog Who Couldn't Stop Loving: How Dogs Have Captured Our Hearts for Thousands of YearsNo ratings yet
- Edward's Menagerie: Dogs: 50 canine crochet patternsFrom EverandEdward's Menagerie: Dogs: 50 canine crochet patternsRating: 3 out of 5 stars3/5 (5)
- Your Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesFrom EverandYour Dog Is Your Mirror: The Emotional Capacity of Our Dogs and OurselvesRating: 4 out of 5 stars4/5 (31)
- Animals Make Us Human: Creating the Best Life for AnimalsFrom EverandAnimals Make Us Human: Creating the Best Life for AnimalsRating: 4.5 out of 5 stars4.5/5 (2)
- I Am Bunny: How a ""Talking"" Dog Taught Me Everything I Need to Know About Being HumanFrom EverandI Am Bunny: How a ""Talking"" Dog Taught Me Everything I Need to Know About Being HumanRating: 4.5 out of 5 stars4.5/5 (8)
- Our Dogs, Ourselves: The Story of a Singular BondFrom EverandOur Dogs, Ourselves: The Story of a Singular BondRating: 4 out of 5 stars4/5 (21)
- Puppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!From EverandPuppy Training 101: How to Train a Puppy, Training Your Own Psychiatric Service Dog, A Step-By-Step Program so your Pup Will Understand You!Rating: 5 out of 5 stars5/5 (85)
- Arthur: The Dog Who Crossed the Jungle to Find a HomeFrom EverandArthur: The Dog Who Crossed the Jungle to Find a HomeRating: 4.5 out of 5 stars4.5/5 (20)
- What Cats Want: An Illustrated Guide for Truly Understanding Your CatFrom EverandWhat Cats Want: An Illustrated Guide for Truly Understanding Your CatRating: 4.5 out of 5 stars4.5/5 (13)
- How to Be Your Dog's Best Friend: A Training Manual for Dog ownersFrom EverandHow to Be Your Dog's Best Friend: A Training Manual for Dog ownersRating: 4 out of 5 stars4/5 (120)