You might also like
- Respiratory Distress SyndromeDocument10 pagesRespiratory Distress SyndromeKomang Rendy KrisnadiNo ratings yet
- Respiratory Distress SyndromeDocument9 pagesRespiratory Distress SyndromeIrawati Eka PutriNo ratings yet
- Management of Respiratory Distress Syndrome: An Update: Ricardo J Rodriguez MDDocument9 pagesManagement of Respiratory Distress Syndrome: An Update: Ricardo J Rodriguez MDIndah Afriani NasutionNo ratings yet
- Respiratory Distress Syndrome Ped 401 MLDocument23 pagesRespiratory Distress Syndrome Ped 401 MLWongani ZuluNo ratings yet
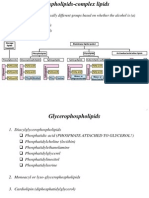
- Phospholipid and Glycolipid MetabolismDocument50 pagesPhospholipid and Glycolipid MetabolismTuğçe Tnc50% (2)
- Respiratory Distress Syndrome in Premature BabiesDocument7 pagesRespiratory Distress Syndrome in Premature BabiesSiti Novita KumanNo ratings yet
- 3RD Lec Pulmonary Surfactant and RDSDocument40 pages3RD Lec Pulmonary Surfactant and RDSIbrahim MigdadyNo ratings yet
- Surfactantreplacementtherapy 160926164838Document33 pagesSurfactantreplacementtherapy 160926164838revathidadam55555No ratings yet
- Fetal Lung MaturityDocument10 pagesFetal Lung MaturityAtika SugiartoNo ratings yet
- Enf Membrana HialinaDocument13 pagesEnf Membrana HialinaAlejandra MedinaNo ratings yet
- Respiratory Distress Syndrome - MBCHBDocument23 pagesRespiratory Distress Syndrome - MBCHBMalueth AnguiNo ratings yet
- Surf Act Ant ReplacementDocument28 pagesSurf Act Ant Replacementapi-27504339100% (3)
- CASE 1: Manipac Yao: Cmmatias (Cmed 2022)Document3 pagesCASE 1: Manipac Yao: Cmmatias (Cmed 2022)Charm MatiasNo ratings yet
- Embryonic 8wks (3-7wks) Lung Hypoplasia, TEF Pseudoglandular 16 Wks CDH Canalicular 24 Wks Surfactant def-RDSDocument40 pagesEmbryonic 8wks (3-7wks) Lung Hypoplasia, TEF Pseudoglandular 16 Wks CDH Canalicular 24 Wks Surfactant def-RDSMischief ManagerNo ratings yet
- Surfactant Replacement Therapy: From Biological Basis To Current Clinical PracticeDocument8 pagesSurfactant Replacement Therapy: From Biological Basis To Current Clinical PracticeBetharia TriayuNo ratings yet
- RDS Ppts 2021Document37 pagesRDS Ppts 2021Mohammad NajjarNo ratings yet
- Hyaline Membrane Disease (HMD) : The Role of The Perinatal PathologistDocument9 pagesHyaline Membrane Disease (HMD) : The Role of The Perinatal PathologistDesyAyu DzulfaAry EomutNo ratings yet
- Metabolic Precursors of SurfactantDocument8 pagesMetabolic Precursors of Surfactantatika sgrtNo ratings yet
- Prematures With Respiratory Distress Syndrome Do Not Have Increased The Chance of Patent Ductus Arteriosus Requiring Indomethacin Therapy ThereafterDocument58 pagesPrematures With Respiratory Distress Syndrome Do Not Have Increased The Chance of Patent Ductus Arteriosus Requiring Indomethacin Therapy ThereafterAndy SungNo ratings yet
- MCN Final Topic 2Document17 pagesMCN Final Topic 2Salea Fleur TaverronNo ratings yet
- Idiopathic Respiratory Disease SyndromeDocument30 pagesIdiopathic Respiratory Disease SyndromeAllan-VonNo ratings yet
- p53 ProliferDocument12 pagesp53 Prolifertest2012No ratings yet
- Phoospoliapase Anti CovidDocument17 pagesPhoospoliapase Anti CovidYudha SatriaNo ratings yet
- Pulmonary SystemDocument19 pagesPulmonary SystemKhushiNo ratings yet
- Surfactant PresentationDocument18 pagesSurfactant PresentationMaadaNo ratings yet
- Eni Rahmawati, S.Kep., NS., M.KepDocument46 pagesEni Rahmawati, S.Kep., NS., M.KepLisa Qoriana RohmaniNo ratings yet
- Hyaline Membrane DiseaseDocument14 pagesHyaline Membrane DiseaseagusNo ratings yet
- Infant Respiratory Distress Syndrome (Irds)Document24 pagesInfant Respiratory Distress Syndrome (Irds)aalfitayahNo ratings yet
- Respiratory Distress SyndromeDocument7 pagesRespiratory Distress SyndromeBilal RowaihiNo ratings yet
- Respiratory Distress Syndrome (RDS) GuideDocument18 pagesRespiratory Distress Syndrome (RDS) GuideMaricel DefiestaNo ratings yet
- Respiratory Distress SyndromeDocument30 pagesRespiratory Distress SyndromeDennis MiritiNo ratings yet
- Common Neonatal Disorders 3Document25 pagesCommon Neonatal Disorders 3Laishram Deeva ChanuNo ratings yet
- Respiratory Distress SyndromeDocument3 pagesRespiratory Distress SyndromeAshNo ratings yet
- Update in Surfactant TherapyDocument12 pagesUpdate in Surfactant TherapyGun HawkNo ratings yet
- Structures of Some Common PhospholipidsDocument9 pagesStructures of Some Common PhospholipidsAdina AhmetovicNo ratings yet
- Respiratory Distress Syndrome: NewbornDocument17 pagesRespiratory Distress Syndrome: NewbornLoloNo ratings yet
- Pediatrics Exposition.: Pulmonary Respiratory Pathology in Preterm Infants (Under 37 Weeks of Gestation)Document2 pagesPediatrics Exposition.: Pulmonary Respiratory Pathology in Preterm Infants (Under 37 Weeks of Gestation)David Rodríguez GarcíaNo ratings yet
- 4 Respiratory Distress Syndrome in The NewbornDocument3 pages4 Respiratory Distress Syndrome in The NewbornChristine Danica BiteraNo ratings yet
- Respiratory Distress Syndrome in NewbornDocument24 pagesRespiratory Distress Syndrome in NewbornDrRajneesh Shastri100% (1)
- Direct Observation of The Coexistence of Two Fluid Phases in Native Pulmonary Surfactant Membranes at Physiological TemperaturesDocument9 pagesDirect Observation of The Coexistence of Two Fluid Phases in Native Pulmonary Surfactant Membranes at Physiological TemperaturesFadi Simon de Souza MagalhãesNo ratings yet
- Surfactan Therapy For NeonatesDocument20 pagesSurfactan Therapy For Neonatesfarah1218No ratings yet
- Intensive Care Nursery House Staff ManualDocument9 pagesIntensive Care Nursery House Staff ManualVenus MargaretteNo ratings yet
- Continuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress SyndromeDocument4 pagesContinuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress Syndromelaudya100% (1)
- Role of pulmonary surfactant components in surface film formationDocument16 pagesRole of pulmonary surfactant components in surface film formationramesh guptaNo ratings yet
- Pulmonary Physiology of The NewbornDocument39 pagesPulmonary Physiology of The NewbornADNo ratings yet
- Respiratory/Integumentary Student Learning OutcomesDocument7 pagesRespiratory/Integumentary Student Learning OutcomesKelsey WallaceNo ratings yet
- The Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceDocument12 pagesThe Cell Cycle Inhibitor P21 Promotes The Development of - 2022 - Acta PharmaceMohammed Shuaib AhmedNo ratings yet
- Warren 2009 RDSDocument13 pagesWarren 2009 RDSCIRUABCNo ratings yet
- Dr. M. Azhar Chishti Dept. Medical BiochemistryDocument46 pagesDr. M. Azhar Chishti Dept. Medical Biochemistryvarsha CRNo ratings yet
- HIF pathway suppression by hypercapniaDocument9 pagesHIF pathway suppression by hypercapniaAnonymous i71HvPXNo ratings yet
- Optimal Oxygenation and Role of Free Radicals in PPHNDocument26 pagesOptimal Oxygenation and Role of Free Radicals in PPHNJessica SofianNo ratings yet
- o Reilly Thébaud 2014 Animal Models of Bronchopulmonary Dysplasia the Term Rat Models 1Document11 pageso Reilly Thébaud 2014 Animal Models of Bronchopulmonary Dysplasia the Term Rat Models 1alihamraghaniNo ratings yet
- Pathophysiology of Apnea, Hypoxia, andDocument35 pagesPathophysiology of Apnea, Hypoxia, andChethan UpadhyayaNo ratings yet
- Phospholipids Across Scales: Lipid Patterns and Plant DevelopmentDocument20 pagesPhospholipids Across Scales: Lipid Patterns and Plant DevelopmentAswad ZEllzNo ratings yet
- Ijms-21-03075 IniDocument14 pagesIjms-21-03075 IniMila KarmilaNo ratings yet
- Respiratory Burst 1 PDFDocument11 pagesRespiratory Burst 1 PDFBasilio Papuico RomeroNo ratings yet
- Aiims - Pediatrics Q&ADocument207 pagesAiims - Pediatrics Q&AqqypprcyxyNo ratings yet
- 1 Respiratory DiseasesDocument22 pages1 Respiratory Diseasesalielabadi10No ratings yet
- Cafeina ArandaDocument14 pagesCafeina ArandaFer Fed GaNo ratings yet
- Pulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungFrom EverandPulmonary Endocrine Pathology: Endocrine Cells and Endocrine Tumours of the LungNo ratings yet
- Quality Agreement Guideline - Final - December 2009 - Clean PDFDocument52 pagesQuality Agreement Guideline - Final - December 2009 - Clean PDFflongNo ratings yet
- Bronchoobstrustive SyndromeDocument32 pagesBronchoobstrustive SyndromeCk Kma67% (3)
- Abs Bench 500 Manual 3esDocument15 pagesAbs Bench 500 Manual 3esmaremotusNo ratings yet
- Univan Maritime (H.K.) Limited: Rug and Alcohol Olicy EctionDocument1 pageUnivan Maritime (H.K.) Limited: Rug and Alcohol Olicy Ectionnavigator1977No ratings yet
- Vital Signs: Measurements of Basic Body FunctionsDocument175 pagesVital Signs: Measurements of Basic Body FunctionsrnrmmanphdNo ratings yet
- Tilapia 4Document69 pagesTilapia 4Annisa MeilaniNo ratings yet
- 2.1.1.1. Aguilar and Stiles' Experiment.: Visual Adaptation and Retinal G A I N Controls 2 7 7Document1 page2.1.1.1. Aguilar and Stiles' Experiment.: Visual Adaptation and Retinal G A I N Controls 2 7 7AkicaNo ratings yet
- Research About Tuba TubaDocument20 pagesResearch About Tuba Tubakoala1388No ratings yet
- Untitled 25Document530 pagesUntitled 25Tony ChangNo ratings yet
- Congenital Adrenal HyperplasiaDocument5 pagesCongenital Adrenal HyperplasiaduapajNo ratings yet
- SonoAce R5 Reference Manual P PDFDocument150 pagesSonoAce R5 Reference Manual P PDFNeto Infomab MedNo ratings yet
- 2014 Bulletin 492Document79 pages2014 Bulletin 492Alexandra CrăciunNo ratings yet
- UAE HospitalsDocument20 pagesUAE Hospitalsswati_progNo ratings yet
- The Scoring Clinical Index For OnychomycosisDocument4 pagesThe Scoring Clinical Index For OnychomycosisPatricia Avalos C.No ratings yet
- Age in A Graying America: Numbers, Profiles, Trends: Nicholas Collins PA-C With Thanks To Diana Koin, M.DDocument42 pagesAge in A Graying America: Numbers, Profiles, Trends: Nicholas Collins PA-C With Thanks To Diana Koin, M.DVidya BalaNo ratings yet
- ) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10Document2 pages) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10swapnil goyalNo ratings yet
- Cyst of Jaws-RadiologyDocument60 pagesCyst of Jaws-RadiologyshabeelpnNo ratings yet
- Implantology Made Easy, 1ed (2008)Document329 pagesImplantology Made Easy, 1ed (2008)Daniel RapcauNo ratings yet
- Code & Ra 9173Document9 pagesCode & Ra 9173Bryan NorwayneNo ratings yet
- Anti-Dopamine D2 Receptor Antibody Ab30743 Anti-Dopamine D2 Receptor Antibody Ab30743Document3 pagesAnti-Dopamine D2 Receptor Antibody Ab30743 Anti-Dopamine D2 Receptor Antibody Ab30743Michael DaleyNo ratings yet
- Primer MSDS Safety Data For AmmoniaDocument26 pagesPrimer MSDS Safety Data For AmmoniaМилутин ШишмановићNo ratings yet
- PHA070 SAS 3 Medication Error 2Document8 pagesPHA070 SAS 3 Medication Error 2jenet soleilNo ratings yet
- FPC Manual PDFDocument75 pagesFPC Manual PDFD'Shea OllivierreNo ratings yet
- ResuscitationDocument38 pagesResuscitationsonics issacNo ratings yet
- Meet B.G.: A Nutrition Care Plan by Michelle SartaDocument14 pagesMeet B.G.: A Nutrition Care Plan by Michelle Sartaapi-340851914No ratings yet
- All Important Diagrams Class 10 (Prashant Kirad) PDFDocument39 pagesAll Important Diagrams Class 10 (Prashant Kirad) PDFharshita1934100% (1)
- Hip Alert ProcessDocument1 pageHip Alert Processapi-264494543No ratings yet
- PDCADocument8 pagesPDCAHendro DimedjoNo ratings yet
- Fluoride and Fluoridation: Topical FluoridesDocument3 pagesFluoride and Fluoridation: Topical FluoridesmarkoNo ratings yet
- JC - Endoscopic Techniques in OralDocument33 pagesJC - Endoscopic Techniques in OralNarla SusheelNo ratings yet