You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Maybury ManualDocument55 pagesMaybury ManualFriends of MayburyNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Musculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324Document8 pagesMusculoskeletal System (20000 Series) : A) 20205 B) 20206 C) 20225 D) 27324JJKNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoNo ratings yet
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoNo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
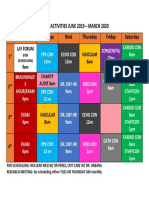
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Research ProtocolDocument13 pagesResearch ProtocolReda SoNo ratings yet
- IungDocument8 pagesIungReda SoNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- 7.3. Obat StimulanDocument16 pages7.3. Obat StimulanLaras OktavianiNo ratings yet
- Impaired Swallowing Care PlanDocument5 pagesImpaired Swallowing Care Planjakifer33% (3)
- Bayabas: Instructions For GuavaDocument2 pagesBayabas: Instructions For GuavadorothypearlNo ratings yet
- Analisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaDocument7 pagesAnalisis Kesesuaian Penggunaan Antiinfeksi Pada Infeksi Oportunistik Pasien Hiv/Aids Rawat Inap Di Rsup Dr. Sardjito YogyakartaindahNo ratings yet
- KC Basic English 2021Document11 pagesKC Basic English 2021ShafanaiNo ratings yet
- INTRODUCTIONDocument3 pagesINTRODUCTIONSoumya Suguna TripathyNo ratings yet
- Ivt BTDocument3 pagesIvt BTAB AlmazoraNo ratings yet
- Theragran (Multiple Vitamins)Document3 pagesTheragran (Multiple Vitamins)Adrianne BazoNo ratings yet
- JDO 50 Non-Extraction Treatment of Pseudo Class III Anterior Cross BiteDocument17 pagesJDO 50 Non-Extraction Treatment of Pseudo Class III Anterior Cross BiteLiying JuNo ratings yet
- HSV1 HSV2 R-Gene & VZV R-GeneDocument2 pagesHSV1 HSV2 R-Gene & VZV R-GeneSachinNo ratings yet
- Clinical Features, Etiologies, and Outcomes in Adult Patients WithDocument13 pagesClinical Features, Etiologies, and Outcomes in Adult Patients Withagarrido2No ratings yet
- Nursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalDocument334 pagesNursing Procedure Manual Nobel Medical College Teaching Hospital Biratnager, NepalSweta ManandharNo ratings yet
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: Pharmacology and Toxicology PracticalDocument2 pagesDr. Naitik D Trivedi & Dr. Upama N. Trivedi: Pharmacology and Toxicology PracticalAnjali RaulNo ratings yet
- Umblical Cord AbnormalitiesDocument54 pagesUmblical Cord AbnormalitiesKeerti Patel100% (5)
- Management of Anembryonic Pregnancy Loss: An Observational StudyDocument6 pagesManagement of Anembryonic Pregnancy Loss: An Observational StudyAnonymous ORleRrNo ratings yet
- Medical Terminology Express A Short Course Approach by Body System 2Nd Edition Gylys Test Bank Full Chapter PDFDocument34 pagesMedical Terminology Express A Short Course Approach by Body System 2Nd Edition Gylys Test Bank Full Chapter PDFDebraBurtonkfman100% (12)
- Department of Clinical Medicine and SurgeryDocument2 pagesDepartment of Clinical Medicine and SurgeryBonface KenaniNo ratings yet
- PRO III 2012 Long Case (Surgical)Document39 pagesPRO III 2012 Long Case (Surgical)vijayaNo ratings yet
- Blood Collection TubesDocument1 pageBlood Collection TubesMohammad Atiq100% (1)
- TFCBT Training GuidelinesDocument3 pagesTFCBT Training GuidelinespolNo ratings yet
- Antibiotic Decision Making in IcuDocument11 pagesAntibiotic Decision Making in IcumalvindersahiNo ratings yet
- Module 5 - Formative Assessment 10 - NCM 112 CARE OF CLIENTS WITH PROBLEMS IN OXYGFENATION FLUDocument9 pagesModule 5 - Formative Assessment 10 - NCM 112 CARE OF CLIENTS WITH PROBLEMS IN OXYGFENATION FLUDharylle CariñoNo ratings yet
- Health Benefits of Bicycle RidingDocument3 pagesHealth Benefits of Bicycle RidingPeter JohnsonNo ratings yet
- Negative Inspiratory Pressure As A Predictor of Weaning Mechanical VentilationDocument3 pagesNegative Inspiratory Pressure As A Predictor of Weaning Mechanical VentilationamonlisaNo ratings yet
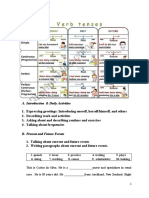
- Tugas 1 Writing 4-Bing4309Document1 pageTugas 1 Writing 4-Bing4309DitaSariKusumaNo ratings yet
- Age EstimatiDocument4 pagesAge EstimatimkumNo ratings yet
- CDC 26714 DS1Document383 pagesCDC 26714 DS1Joyce AngobungNo ratings yet
- DVH LimitsDocument1 pageDVH LimitsDioni SandovalNo ratings yet