You might also like
- Welcome Plan Welcome CorpsDocument20 pagesWelcome Plan Welcome CorpsAxmed Cadnaan50% (2)
- Cardiovascular System: Mungcal, Dharlynette RTRPDocument77 pagesCardiovascular System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanNo ratings yet
- Interview-Questions (ADNOC LNG)Document19 pagesInterview-Questions (ADNOC LNG)Chen XinNo ratings yet
- Anesthesia for Congenital Heart DiseaseFrom EverandAnesthesia for Congenital Heart DiseaseStephen A. StayerNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Rhythm Control Versus Rate Control in Atrial Fibrillation - UpToDocument39 pagesRhythm Control Versus Rate Control in Atrial Fibrillation - UpTohatsune100% (1)
- LTF InterpretationDocument3 pagesLTF InterpretationkiethyanNo ratings yet
- Use of Vasopressors and Inotropes - UpToDateDocument18 pagesUse of Vasopressors and Inotropes - UpToDateAlbertoMarteNo ratings yet
- Atrial Fibrillation and Flutter After Cardiac Surgery - UpToDateDocument22 pagesAtrial Fibrillation and Flutter After Cardiac Surgery - UpToDateFlavia SaccomaniNo ratings yet
- Heart DiseaseDocument38 pagesHeart DiseaseDr.Sunil KumarNo ratings yet
- Prevention of DVT/PE: Noornadia BT Yahaya 050100841Document32 pagesPrevention of DVT/PE: Noornadia BT Yahaya 050100841Nadia YahayaNo ratings yet
- Left Ventricular Assist DevicesDocument14 pagesLeft Ventricular Assist DevicesLuis Alberto Caneo VergaraNo ratings yet
- Acls Course HandoutsDocument8 pagesAcls Course HandoutsRoxas CedrickNo ratings yet
- Acute Heart FailureDocument71 pagesAcute Heart FailureVivek Anandan100% (1)
- HW InotropesDocument3 pagesHW InotropesNatalie YeohNo ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- Dysrhythmias: Sinus Node Dysrhythmias Tachycardia, and Sinus ArrhythmiaDocument5 pagesDysrhythmias: Sinus Node Dysrhythmias Tachycardia, and Sinus ArrhythmiaKayelyn-Rose Combate100% (1)
- Approach To The Patient With Respiratory DiseaseDocument6 pagesApproach To The Patient With Respiratory DiseaseRem AlfelorNo ratings yet
- Cerebrovascular AccidentDocument31 pagesCerebrovascular AccidentRam ReddyNo ratings yet
- Acid-Base BalanceDocument5 pagesAcid-Base BalanceCarl Earvin L. FavoritoNo ratings yet
- HANDOUTS-Non Invasive VentilationDocument15 pagesHANDOUTS-Non Invasive VentilationKristine MangasepNo ratings yet
- PFT Interpretation AlgorithmDocument4 pagesPFT Interpretation AlgorithmJason Steel50% (2)
- Ischemic Heart DiseaseDocument28 pagesIschemic Heart DiseaseLiusHarimanNo ratings yet
- Cardiac Output and Hemodynamic MeasurementDocument29 pagesCardiac Output and Hemodynamic Measurementdeepa100% (1)
- ASCITESDocument25 pagesASCITESGanesh BabuNo ratings yet
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNo ratings yet
- 01 Hypertension - 2019 2020 PDFDocument122 pages01 Hypertension - 2019 2020 PDFbaraa abu sneineh100% (1)
- Renal - Replacement - TherapyDocument128 pagesRenal - Replacement - TherapyEmNo ratings yet
- Mitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationDocument33 pagesMitral Valve Prolapse, Flailed Mitral Valve Mitral Annular CalcificationcafemedNo ratings yet
- Acs Nstemi PathwayDocument3 pagesAcs Nstemi PathwayAliey's SKeplek NgeNersNo ratings yet
- Pakrat 10Document67 pagesPakrat 10towexpertNo ratings yet
- Acid-Base Disorders NotesDocument10 pagesAcid-Base Disorders NotesLovely100% (1)
- How To Treat: Septic ShockDocument6 pagesHow To Treat: Septic ShockmeeandsoeNo ratings yet
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 pagesVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNo ratings yet
- Treatment of Resistant and Refractory HypertensionDocument21 pagesTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Ch-13 Drugs Used in Heart FailureDocument49 pagesCh-13 Drugs Used in Heart FailureShabrin SadikhNo ratings yet
- Milrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1Document1 pageMilrinone Can ONLY Be Mixed With NS!: Alpha 1 Beta 1 & Alpha 1njones33No ratings yet
- VasculitidesDocument13 pagesVasculitidesIrene Zae MwandotoNo ratings yet
- Valvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyDocument44 pagesValvular Heart Disease and Non Cardiac Surgery: Lakshmi P. YalavarthyLakshmi YalavarthyNo ratings yet
- MayoclinprocDocument12 pagesMayoclinprocpriyaNo ratings yet
- COPD Updated Guidelines and Newer TherapiesDocument90 pagesCOPD Updated Guidelines and Newer TherapiesVlad Constantin100% (1)
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- DO /VO Relationships: J. L. VincentDocument8 pagesDO /VO Relationships: J. L. VincentLucas Cárcamo SaavedraNo ratings yet
- Clinical Cheat Sheet: Radiographic AssessmentDocument1 pageClinical Cheat Sheet: Radiographic AssessmentTracy PopeNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Pre Assessment Diabetes Nursing CareDocument4 pagesPre Assessment Diabetes Nursing CareHabib UllahNo ratings yet
- Rosenberg Circulatory Assist DevicesDocument61 pagesRosenberg Circulatory Assist DevicesMilisha Albro100% (1)
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Sign and SymptomsDocument8 pagesSign and SymptomsCaral Grace Gatdula-PenalbaNo ratings yet
- 2018 AHA Guidelines BradicardiaDocument106 pages2018 AHA Guidelines BradicardiaArio Richard NinaNo ratings yet
- Left Ventricular Non-CompactionDocument20 pagesLeft Ventricular Non-CompactionlawlietNo ratings yet
- Hemodynamics in The Cath Lab 2Document45 pagesHemodynamics in The Cath Lab 2usfcards100% (1)
- Guidelines For Platelet Transfusions in Dengue FeverDocument4 pagesGuidelines For Platelet Transfusions in Dengue FeverGuru Prasad100% (1)
- Cardiac - Potpourri Rev 2015Document80 pagesCardiac - Potpourri Rev 2015Sanaz NikiNo ratings yet
- S1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesDocument10 pagesS1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesCHARIEMAE CA�AZARESNo ratings yet
- Pericarditis 65 SlidesDocument65 pagesPericarditis 65 SlidesAtifBhoreNo ratings yet
- Lecture 4: Hypovolemic ShockDocument20 pagesLecture 4: Hypovolemic Shockj.doe.hex_87No ratings yet
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
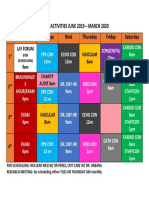
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- Research ProtocolDocument13 pagesResearch ProtocolReda SoNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoNo ratings yet
- IungDocument8 pagesIungReda SoNo ratings yet
- Punjab Medicolegal Manual Jan30 PDFDocument18 pagesPunjab Medicolegal Manual Jan30 PDFFrank NobodNo ratings yet
- Application Form - FMU (New Form BUPA)Document16 pagesApplication Form - FMU (New Form BUPA)gabinicolescu9999No ratings yet
- Autism PDFDocument25 pagesAutism PDFTalal 197No ratings yet
- 04telkom OkDocument248 pages04telkom OksilvaniNo ratings yet
- A - Pratic Guide Pediatric Wound CareDocument9 pagesA - Pratic Guide Pediatric Wound CareLicia GabrielleNo ratings yet
- Personal Development: Performance TaskDocument3 pagesPersonal Development: Performance TaskharrygolunaNo ratings yet
- Surveying Lab Manual 21cv32 - 2022Document82 pagesSurveying Lab Manual 21cv32 - 2022Tamil Selvi CIVILNo ratings yet
- PCT For BodybuildersDocument12 pagesPCT For BodybuildersJon Mester100% (4)
- Biotech SyllabusDocument2 pagesBiotech Syllabusmeet2abhayNo ratings yet
- AcuitSign M8&M6&M5&M3 User's Manual 20141215 - CompressedDocument305 pagesAcuitSign M8&M6&M5&M3 User's Manual 20141215 - CompressedElectromedycal EQUIPO MEDICONo ratings yet
- Reading and Writing - q3 - Las 1-2 RTPDocument4 pagesReading and Writing - q3 - Las 1-2 RTPRenz Ian T. DacoronNo ratings yet
- Makassar 1: Total Target OptimisDocument2 pagesMakassar 1: Total Target OptimisAchaElmanNo ratings yet
- Mil PRF 680CDocument12 pagesMil PRF 680CfltpNo ratings yet
- OSCE Checklist Cervical Screening SmearDocument2 pagesOSCE Checklist Cervical Screening SmearNoreen Hannah GabrielNo ratings yet
- Erich Fromm - A Therapeutic Vision Well Ahead of Its TimeDocument8 pagesErich Fromm - A Therapeutic Vision Well Ahead of Its TimeSteluța DrâmbuNo ratings yet
- TOK SampleDocument5 pagesTOK SampleLucianna CheilasNo ratings yet
- THE - Jose SILVA - METHODDocument43 pagesTHE - Jose SILVA - METHODszijsaNo ratings yet
- Sonography ProjectDocument9 pagesSonography Projectapi-685351719No ratings yet
- Time Management Training by Lisa J DownsDocument6 pagesTime Management Training by Lisa J DownssoberNo ratings yet
- InformationDocument3 pagesInformationابراهيم عماد نجم محمدNo ratings yet
- CS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalDocument1 pageCS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalRavi Parhar75% (4)
- New Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Document132 pagesNew Harbinger Self-Help Workbook the Mindfulness and Acceptance Workbook for Social Anxiety and Shyness_ Using Acceptance and Commitment Therapy to Free Yourself From Fear and Reclaim Your Life [1st Ed.Wesley Ramalho100% (1)
- Food Safety Is Everybody's Responsibility: PhilippinesDocument3 pagesFood Safety Is Everybody's Responsibility: PhilippinesMa. Regina GasparNo ratings yet
- Sample File: Lamentations Flame PrincessDocument5 pagesSample File: Lamentations Flame PrincessBraunerNo ratings yet
- Agricultural Stage Agriculture Was Started Affecting SoDocument8 pagesAgricultural Stage Agriculture Was Started Affecting Soyangi dokaNo ratings yet
- Gallucci (2004) - Immediate Loading With Fixed Screw-Retained Provisional Restorations in Edentulous Jaws, The Pickup Technique.Document10 pagesGallucci (2004) - Immediate Loading With Fixed Screw-Retained Provisional Restorations in Edentulous Jaws, The Pickup Technique.Antonio González Ruiz0% (1)
- Health Education of Menstrual Hygiene 1Document12 pagesHealth Education of Menstrual Hygiene 1chaudharitrushar007No ratings yet
- Personal Hygiene Kit Product Details PDFDocument3 pagesPersonal Hygiene Kit Product Details PDFZulfirdaus A'AdnanNo ratings yet