You might also like
- Deep Venous ThrombosisDocument7 pagesDeep Venous ThrombosisUzma KhanNo ratings yet
- Thrombo Embolism and PregnancyDocument9 pagesThrombo Embolism and Pregnancysangeetha francisNo ratings yet
- Clinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Surgery Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2No ratings yet
- Venous Thromboembolism in Pregnancy: EpidemiologyDocument8 pagesVenous Thromboembolism in Pregnancy: EpidemiologyKhalil KhusairiNo ratings yet
- VTEDocument45 pagesVTEABREHAM BUKULONo ratings yet
- Deep Vein Thrombosis & Its ProphylaxisDocument90 pagesDeep Vein Thrombosis & Its ProphylaxisPratik KumarNo ratings yet
- Thromboembolic DisordersDocument6 pagesThromboembolic DisordersadiNo ratings yet
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Coagulation Disorders in ObsDocument33 pagesCoagulation Disorders in Obsapule geraldhumbleNo ratings yet
- Venous ThromboembolismDocument6 pagesVenous ThromboembolismAkhilaNo ratings yet
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Pharmacotherapy of VTEDocument80 pagesPharmacotherapy of VTEAbera JamboNo ratings yet
- Friedman VTE Bundle PDFDocument24 pagesFriedman VTE Bundle PDFGerman Parra CNo ratings yet
- Thrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Document39 pagesThrombophl Ebitis: Santos, Maria Ericka B. BSN Iii - 1Ericka SantosNo ratings yet
- Postpartum CollapseDocument54 pagesPostpartum Collapsemedical chroniclesNo ratings yet
- DVT by DR KabareDocument24 pagesDVT by DR KabareAustine OdhiamboNo ratings yet
- Deep Vein ThrombosisDocument22 pagesDeep Vein ThrombosisEznal MahidinNo ratings yet
- Non Pharmacological Method For Prevention and Treatment ofDocument34 pagesNon Pharmacological Method For Prevention and Treatment ofBhaskar Borgohain100% (2)
- Clinical Diagnosis ofDocument14 pagesClinical Diagnosis ofNor Shuhada HaronNo ratings yet
- Liver Cancer Diagnosis & Treatment Options Under 40 CharactersDocument5 pagesLiver Cancer Diagnosis & Treatment Options Under 40 CharactersSheryl OcampoNo ratings yet
- Nonpharmacological Prophylaxis of DVT: SriherDocument32 pagesNonpharmacological Prophylaxis of DVT: SriherDwi ayu widiariniNo ratings yet
- VTE Deep Vein Thrombosis Pulmonary Embolism: Wong Cai Hui Supervisor: DR PradeepDocument75 pagesVTE Deep Vein Thrombosis Pulmonary Embolism: Wong Cai Hui Supervisor: DR PradeepALIF HAIQAL MOHD HUSSEINNo ratings yet
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- THROMBOPHLEBITISDocument50 pagesTHROMBOPHLEBITISmers puno100% (3)
- Anticoagulation in PregnancyDocument8 pagesAnticoagulation in PregnancyEdwin BravoNo ratings yet
- Postpartum Haemorrhage (Edited)Document37 pagesPostpartum Haemorrhage (Edited)kibreabsello4No ratings yet
- DEEP VEIN Dr. Samira BelkheirDocument43 pagesDEEP VEIN Dr. Samira BelkheirkalfNo ratings yet
- Thromoembolic DisordersDocument34 pagesThromoembolic DisordersAhmed AyasrahNo ratings yet
- Early Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskDocument4 pagesEarly Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskAnderson LondoñoNo ratings yet
- Management of Patients With Vascular Disorders: Venous ArterialDocument56 pagesManagement of Patients With Vascular Disorders: Venous ArterialHamss AhmedNo ratings yet
- Updated PE and FESDocument35 pagesUpdated PE and FESNg AliceNo ratings yet
- 18 Nov 2018Document23 pages18 Nov 2018Affy SyifaraniNo ratings yet
- Low Molecular Weight Heparin Guidance for Safe Prescribing in Primary CareDocument33 pagesLow Molecular Weight Heparin Guidance for Safe Prescribing in Primary CareAtikah Putri AtmojoNo ratings yet
- Pulmonary EmbolismDocument46 pagesPulmonary EmbolismAnusha VergheseNo ratings yet
- Coagulation Disorders in PregnancyDocument20 pagesCoagulation Disorders in PregnancyHannaTashiaClaudiaNo ratings yet
- GUIDELINES FOR PREVENTING VENOUS THROMBOEMBOLISMDocument26 pagesGUIDELINES FOR PREVENTING VENOUS THROMBOEMBOLISMRandilufti SantosoNo ratings yet
- Case 9: Deep Vein ThrombosisDocument5 pagesCase 9: Deep Vein Thrombosisintrovoyz041No ratings yet
- VTE Risk Assessment: DR Roopen AryaDocument26 pagesVTE Risk Assessment: DR Roopen AryaA.h.MuradNo ratings yet
- Swelling in LegDocument3 pagesSwelling in LegNeeraj SethiNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Kuliah Thrombosis 2015 NNDocument39 pagesKuliah Thrombosis 2015 NNBeladiena Citra SiregarNo ratings yet
- Venous ThromboemboslimDocument22 pagesVenous ThromboemboslimTitusNo ratings yet
- HAUT HMV Brazil Grand Rounds April 29 2014Document74 pagesHAUT HMV Brazil Grand Rounds April 29 2014carlosrschusterNo ratings yet
- Comparison of Warfarin and Heparin For Thromboprophylaxes Based Upon There Safety, Efficacy and TolerabilityDocument55 pagesComparison of Warfarin and Heparin For Thromboprophylaxes Based Upon There Safety, Efficacy and Tolerabilitysaleemandsons4210No ratings yet
- Casepresentationondvt1 200731074511Document21 pagesCasepresentationondvt1 200731074511alvin.de.fieryNo ratings yet
- Acute Pulmonary Embolism Diagnosis and TreatmentDocument54 pagesAcute Pulmonary Embolism Diagnosis and TreatmentDragan YottNo ratings yet
- Peripheral Vascular Disorders Venous ThrombosisDocument32 pagesPeripheral Vascular Disorders Venous ThrombosisMarlene MathewNo ratings yet
- Thromboembolism & ThromboprophylaxisDocument48 pagesThromboembolism & Thromboprophylaxisazida90No ratings yet
- Venous Thromboembolism Disease Risks, Symptoms and TreatmentDocument25 pagesVenous Thromboembolism Disease Risks, Symptoms and TreatmentOmar AbdillahiNo ratings yet
- Anaesthesia For Non Obstetric Surgeries in Pregnant PatientsDocument35 pagesAnaesthesia For Non Obstetric Surgeries in Pregnant Patientshell riderNo ratings yet
- Clinical: Section 3 of 10Document36 pagesClinical: Section 3 of 10coleNo ratings yet
- Pre and Post Operative CareDocument9 pagesPre and Post Operative CareSara Abdi OsmanNo ratings yet
- Pulmonary Embolism and Fat Embolism SyndromeDocument37 pagesPulmonary Embolism and Fat Embolism SyndromeAlice HuiiNo ratings yet
- 440 - Med Surg HESI 2Document8 pages440 - Med Surg HESI 2Chalcey Polson87% (15)
- Puerperal Venous ThrombosisDocument25 pagesPuerperal Venous ThrombosisAnitha ThankappanNo ratings yet
- 62 PPH Including Coagulation Failure in ObstetDocument46 pages62 PPH Including Coagulation Failure in ObstetcollinsmagNo ratings yet
- Short Answer Questions AnaesthesiaDocument91 pagesShort Answer Questions AnaesthesiaMeena Ct100% (11)
- Rajalakshmi Engineering CollegeDocument2 pagesRajalakshmi Engineering CollegebalaNo ratings yet
- Probability As A General Concept Can Be Defined As The Chance of An Event OccurDocument14 pagesProbability As A General Concept Can Be Defined As The Chance of An Event OccurMuhammad Adnan KhalidNo ratings yet
- LESSON 1 Random-VariablesDocument29 pagesLESSON 1 Random-Variablesnica jane madrigalNo ratings yet
- Aero 12ADocument2 pagesAero 12AIrwin XavierNo ratings yet
- Adjectives AllDocument35 pagesAdjectives AllJOHN SEBASTIAN PARDO LARANo ratings yet
- Case 1Document6 pagesCase 1Rewaa MerwadNo ratings yet
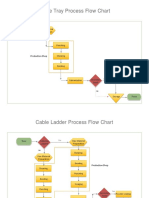
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Quick Manual v2.3: Advanced LTE Terminal With Flexible Inputs ConfigurationDocument16 pagesQuick Manual v2.3: Advanced LTE Terminal With Flexible Inputs ConfigurationanditowillyNo ratings yet
- List of Osho's Complete Audio-Video DVD CollectionDocument15 pagesList of Osho's Complete Audio-Video DVD CollectionOsho Bengaluru100% (2)
- Packing For DeploymentDocument2 pagesPacking For DeploymentMihaila CosminNo ratings yet
- LG Rotary Compressor GuideDocument32 pagesLG Rotary Compressor Guideวรศิษฐ์ อ๋อง33% (3)
- Prota - Stiffness FactorDocument7 pagesProta - Stiffness FactorA K100% (1)
- A 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentDocument9 pagesA 3-Channel Monopulse Tracking Receiver System Using Commercial Off-The-Shelf EquipmentJean-Hubert DelassaleNo ratings yet
- Greenheck Facilities Guide - Locations and Details in Schofield & Mosinee WIDocument1 pageGreenheck Facilities Guide - Locations and Details in Schofield & Mosinee WIRicardo Ruy PeñaNo ratings yet
- Unit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeDocument6 pagesUnit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeJessy RoseNo ratings yet
- Headache PAINDocument1 pageHeadache PAINOmarNo ratings yet
- Project Lakaw: Arduino-base Assisted Stick for Visually Impaired PeopleDocument13 pagesProject Lakaw: Arduino-base Assisted Stick for Visually Impaired PeopleEarl MathewNo ratings yet
- Guitar SetupDocument1 pageGuitar SetupEduardo Maia CardosoNo ratings yet
- Vegan Starter KitDocument53 pagesVegan Starter KitGabriela GarciaNo ratings yet
- Tips On Fatigue - NAVWEPS 00-25-559Document123 pagesTips On Fatigue - NAVWEPS 00-25-559Mark Evan SalutinNo ratings yet
- Those Who Serve - Stephen Melillo (Score)Document22 pagesThose Who Serve - Stephen Melillo (Score)Fernando RamiresNo ratings yet
- Price List Lang Technovation 02072019Document5 pagesPrice List Lang Technovation 02072019api-541004165No ratings yet
- Reflective EssayDocument5 pagesReflective Essaybwood17No ratings yet
- Tribology and Dynamics of Engine and Powertrain Fundamentals Applications and Future TrendsDocument13 pagesTribology and Dynamics of Engine and Powertrain Fundamentals Applications and Future Trendskumar_yogesh2238810% (2)
- Sir James ChadwickDocument6 pagesSir James ChadwickMichael GuevarraNo ratings yet
- Micom P44X: Numerical Distance Protection RelayDocument80 pagesMicom P44X: Numerical Distance Protection RelayKuenley TiNy OndeNo ratings yet
- Liquid Gold Petroleum's Performance and SuccessesDocument2 pagesLiquid Gold Petroleum's Performance and SuccessesShubham DawleNo ratings yet
- STK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverDocument11 pagesSTK6712BMK4: Unipolar Fixed-Current Chopper-Type 4-Phase Stepping Motor DriverGerardo WarmerdamNo ratings yet
- BMW Inyeccion 320i-325i Motronic M31 PDFDocument2 pagesBMW Inyeccion 320i-325i Motronic M31 PDFIvoo ooNo ratings yet
- 2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050Document8 pages2005-2010 Tacoma Bed Extender PT329-35050 Rev. A - PT329-35050kylemac123No ratings yet