You might also like
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 pagesAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNo ratings yet
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- Recent Advances in The Treatment of ShockDocument52 pagesRecent Advances in The Treatment of ShockasupicuNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Pharmacotherapy of heart failureDocument79 pagesPharmacotherapy of heart failureAbera JamboNo ratings yet
- Rheumatic Fever and Rheumatic Heart DiseaseDocument132 pagesRheumatic Fever and Rheumatic Heart DiseaseDamie FernandezNo ratings yet
- Chronic Heart FailureDocument90 pagesChronic Heart FailureTemesgenNo ratings yet
- HF PresentationDocument62 pagesHF Presentationapi-552486649No ratings yet
- The man who wins is the man who thinks he canDocument51 pagesThe man who wins is the man who thinks he cankays30002403No ratings yet
- 2021 CVD Prevention GlsDocument147 pages2021 CVD Prevention GlsRuslan RidcodubskiiNo ratings yet
- Anticoagulants ParamedDocument20 pagesAnticoagulants ParamedManikanta GupthaNo ratings yet
- Pharmacotherapy of Arrythmias For 4th YearDocument79 pagesPharmacotherapy of Arrythmias For 4th Yeartolcharegasa100% (1)
- Necrotizing Fasciitis..By DR Kassahun GirmaDocument49 pagesNecrotizing Fasciitis..By DR Kassahun GirmaKassahun Girma GelawNo ratings yet
- CardiomyopathyDocument8 pagesCardiomyopathyKarisaNo ratings yet
- Advanced Knowledge Assessment in Adult Critical CareDocument570 pagesAdvanced Knowledge Assessment in Adult Critical CareMajor EmadNo ratings yet
- Necrotizing Fasciitis: Early Biopsy Key for Aggressive TreatmentDocument6 pagesNecrotizing Fasciitis: Early Biopsy Key for Aggressive TreatmentVirtues GracesNo ratings yet
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- PPCCMidterm Study Guide 1Document5 pagesPPCCMidterm Study Guide 1Kaitlyn CabreraNo ratings yet
- Acute PancreatitisDocument58 pagesAcute PancreatitissujithNo ratings yet
- First-line heart failure drugs optimize outcomesDocument13 pagesFirst-line heart failure drugs optimize outcomesshinn aikeeNo ratings yet
- Treatment and Classification of Heart FailureDocument2 pagesTreatment and Classification of Heart FailureShannon RamsumairNo ratings yet
- Laboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPDocument41 pagesLaboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPmarieNo ratings yet
- Lymphoma: Pro - Dr.Ahmed EisaDocument45 pagesLymphoma: Pro - Dr.Ahmed EisaOmar Mohammed100% (1)
- Preventive CardiologyDocument28 pagesPreventive CardiologyerizonNo ratings yet
- Anemia 1Document104 pagesAnemia 1maryam ijazNo ratings yet
- Abnormal LFTsDocument2 pagesAbnormal LFTsRenu RosyNo ratings yet
- Anemia Prevention and Management Program Implementation GuideDocument60 pagesAnemia Prevention and Management Program Implementation GuideIchlasul MadriddistaNo ratings yet
- Hypertension LecturesDocument65 pagesHypertension LecturesAdebisiNo ratings yet
- Diseases of The AortaDocument48 pagesDiseases of The AortaYibeltal AssefaNo ratings yet
- 1-History, Evolution and Milestone in PharmacyDocument29 pages1-History, Evolution and Milestone in PharmacyEliza Quines QuizonNo ratings yet
- PLEURAL EFFUSION CAUSES AND DIAGNOSISDocument52 pagesPLEURAL EFFUSION CAUSES AND DIAGNOSISvaishnaviNo ratings yet
- Nephrology WorkbookDocument36 pagesNephrology WorkbookAchrafNo ratings yet
- 01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Document62 pages01-09 2022 Pharm Chronic Care in Cardiology 2022 R4Amira HelayelNo ratings yet
- Cardiovascular Nursing: Study Online atDocument7 pagesCardiovascular Nursing: Study Online atLilly DayeNo ratings yet
- Ch-13 Drugs Used in Heart FailureDocument49 pagesCh-13 Drugs Used in Heart FailureShabrin SadikhNo ratings yet
- Cardiovascular System PDFDocument182 pagesCardiovascular System PDFXochitl ZambranoNo ratings yet
- Diuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamDocument56 pagesDiuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamPrabhakar KumarNo ratings yet
- CVS Examination EditedDocument134 pagesCVS Examination EditedThilak JayalathNo ratings yet
- 2020 ACHD For WebDocument108 pages2020 ACHD For WebRuslan RidcodubskiiNo ratings yet
- Chap253-Heart Failure ManagementDocument42 pagesChap253-Heart Failure ManagementDoctor CastleNo ratings yet
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 pagesClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik BhuvaNo ratings yet
- Blood Vessel Pathologies and VasculitidesDocument13 pagesBlood Vessel Pathologies and VasculitidesIrene Zae MwandotoNo ratings yet
- RBC DisordersDocument19 pagesRBC DisordersAbhiram KrishnaNo ratings yet
- Clinical Lab Hematology: An Overview of Blood Cell AnalysisDocument30 pagesClinical Lab Hematology: An Overview of Blood Cell AnalysisGerald SorianoNo ratings yet
- Evaluation of Chest Pain: Ruling Out Life ThreatsDocument16 pagesEvaluation of Chest Pain: Ruling Out Life ThreatsAbhinit RiddhiNo ratings yet
- Beers CriteriaDocument16 pagesBeers CriteriaNickolasMarllesNo ratings yet
- Valvular Heart DseDocument8 pagesValvular Heart DseJane Pineda CuraNo ratings yet
- Željko Puljiz, MD., PHDDocument67 pagesŽeljko Puljiz, MD., PHDpuljiz7No ratings yet
- 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Top 10 Take-Home MessagesDocument24 pages2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Top 10 Take-Home MessagesAna RuizNo ratings yet
- Introduction To Health Service ManagementDocument70 pagesIntroduction To Health Service ManagementephremNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art Georgesatya_mdsNo ratings yet
- #9 Ie 8 PDFDocument8 pages#9 Ie 8 PDFOmar BasimNo ratings yet
- My Cardiac and Chest SymptomsDocument58 pagesMy Cardiac and Chest SymptomsDhamirah SakinahNo ratings yet
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
- Pharmacology A - Drugs Used in Coagulation CascadeDocument13 pagesPharmacology A - Drugs Used in Coagulation CascadeselflessdoctorNo ratings yet
- 6-8 Thrombolitics Antiplatelet AnticoagulantDocument36 pages6-8 Thrombolitics Antiplatelet AnticoagulantFatima ZahraNo ratings yet
- Atrial FibrillationDocument1 pageAtrial FibrillationCharlie Lee100% (1)
- Bioavailability: by Abera JDocument59 pagesBioavailability: by Abera JAbera JamboNo ratings yet
- 2.2. Physical-Chemical Factors Affecting Oral Absorption (6hrs)Document60 pages2.2. Physical-Chemical Factors Affecting Oral Absorption (6hrs)Abera JamboNo ratings yet
- Pharmacotherapy of Osteoarthritis: Abera J. (Bpharm., MSC in Clinical Pharmacy), School of Pharmacy, CHMS, HuDocument31 pagesPharmacotherapy of Osteoarthritis: Abera J. (Bpharm., MSC in Clinical Pharmacy), School of Pharmacy, CHMS, HuAbera JamboNo ratings yet
- Pharmacotherapy of Gout: A Guide for Managing Acute Attacks and Lowering Uric AcidDocument40 pagesPharmacotherapy of Gout: A Guide for Managing Acute Attacks and Lowering Uric AcidAbera JamboNo ratings yet
- Pharmacotherapy of RADocument44 pagesPharmacotherapy of RAAbera JamboNo ratings yet
- Pharmacotherapy of OsteoporosisDocument49 pagesPharmacotherapy of OsteoporosisAbera JamboNo ratings yet
- Pharmacotherapy of HTNDocument57 pagesPharmacotherapy of HTNAbera JamboNo ratings yet
- Pharmacotherapy of ACSDocument79 pagesPharmacotherapy of ACSAbera JamboNo ratings yet
- Low Molecular Weight Heparins - EN - 24.11.2020Document8 pagesLow Molecular Weight Heparins - EN - 24.11.2020Verónica Isabel Rincón BelandriaNo ratings yet
- Anticoagulant ReversalDocument4 pagesAnticoagulant Reversalapi-647779956No ratings yet
- Euab 065Document65 pagesEuab 065Mathew McCarthyNo ratings yet
- ACS: Acute Coronary SyndromeDocument48 pagesACS: Acute Coronary SyndromeAchmad ulil Albab100% (1)
- Pharmacology of Drugs Used in StrokeDocument93 pagesPharmacology of Drugs Used in StrokemehakNo ratings yet
- Anticoagulation Guidelines JMDocument32 pagesAnticoagulation Guidelines JMMichael HuntNo ratings yet
- The PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismDocument9 pagesThe PERT Concept Q1 A Step-By-Step Approach To Managing Pulmonary EmbolismntnquynhproNo ratings yet
- Periprocedural Anticoagulation Guidelines - UKDocument14 pagesPeriprocedural Anticoagulation Guidelines - UKjoshNo ratings yet
- Acute Coronary Syndrome - 2022Document91 pagesAcute Coronary Syndrome - 2022Rana Khaled AwwadNo ratings yet
- Guidelines For Adult Stroke Rehab and Recovery Ucm 485182Document117 pagesGuidelines For Adult Stroke Rehab and Recovery Ucm 485182Marcelo BenitezNo ratings yet
- Perioperative Care and Management of Complications in Pancreatic SurgeryDocument24 pagesPerioperative Care and Management of Complications in Pancreatic SurgerymshcseNo ratings yet
- Obstetric EmbolismDocument81 pagesObstetric Embolismmiss_izzniNo ratings yet
- Alteration of blood coagulation in CKD patients on dialysisDocument26 pagesAlteration of blood coagulation in CKD patients on dialysissubankar NagNo ratings yet
- Farmakoterapi AntikoagulasiDocument20 pagesFarmakoterapi AntikoagulasiRirin AptNo ratings yet
- Stago CatalogueDocument76 pagesStago CatalogueHary John Tsivery Rakotonjak'sParowNo ratings yet
- 6.drugs For Coagulation Disorders NewDocument24 pages6.drugs For Coagulation Disorders NewNaseem Al tajerNo ratings yet
- Prof DR Akram ICUDocument233 pagesProf DR Akram ICUramzi MohamedNo ratings yet
- 03 Warfarin Pediatric ProtocolDocument2 pages03 Warfarin Pediatric Protocoltl drNo ratings yet
- MoH COVID 19 Protocol - V1.8-1 PDFDocument13 pagesMoH COVID 19 Protocol - V1.8-1 PDFHCX dghhqNo ratings yet
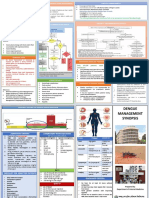
- Dengue Management Synopsis BSMMUDocument2 pagesDengue Management Synopsis BSMMURakibk65No ratings yet
- Cardiology IDocument112 pagesCardiology IAhmad Makhlouf100% (1)
- KDIGO 2012 Clinical Practice Guideline for the Prevention, Detection, Evaluation and Management of Acute Kidney InjuryDocument40 pagesKDIGO 2012 Clinical Practice Guideline for the Prevention, Detection, Evaluation and Management of Acute Kidney InjuryAbedDabajaNo ratings yet
- 1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Document54 pages1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Yathrika YathrikaNo ratings yet
- ORBCON-EN-BE Coagulation 02259Document24 pagesORBCON-EN-BE Coagulation 02259Леон Деспотоски100% (1)
- Cerebral Venous Thrombosis in Sub-Saharan Africa: A Systematic ReviewDocument7 pagesCerebral Venous Thrombosis in Sub-Saharan Africa: A Systematic ReviewDenise MacieNo ratings yet
- UFH LMWH DVT Prophylaxis OverviewDocument2 pagesUFH LMWH DVT Prophylaxis OverviewParvathy R NairNo ratings yet
- 2015 Stago US Product Catalog-DEF-eb PDFDocument44 pages2015 Stago US Product Catalog-DEF-eb PDFDewi PradnyaNo ratings yet
- Peripocedural Anticoagulation LPDocument11 pagesPeripocedural Anticoagulation LPlauraalvisNo ratings yet
- #Davidson - Review #HematologyDocument23 pages#Davidson - Review #Hematologyemtiaz zamanNo ratings yet
- 7: Effective Transfusion in Surgery and Critical CareDocument16 pages7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNo ratings yet