You might also like
- Cowen Therapeutic Outlook March 2009Document1,236 pagesCowen Therapeutic Outlook March 2009Justin LachovskyNo ratings yet
- SMPC LisationDocument4 pagesSMPC LisationRegistrasi FahrenheitNo ratings yet
- Studi Kasus MK Konsep Terapi Genap 2019.2020 - UkbDocument8 pagesStudi Kasus MK Konsep Terapi Genap 2019.2020 - UkbYossi KhrismaeniNo ratings yet
- Alteplase Pharmacokinetics and Thrombolysis RisksDocument24 pagesAlteplase Pharmacokinetics and Thrombolysis Riskssatyagraha84No ratings yet
- Pharmacology of HemostaticDocument6 pagesPharmacology of HemostaticSamuel Dwi WardiyantoNo ratings yet
- Anti Clotting, Fibrinolytic, Tests For CoagulationDocument70 pagesAnti Clotting, Fibrinolytic, Tests For CoagulationDr.Gomathi sivakumarNo ratings yet
- 18.fibrinolytic (Thrombolytic) AgentsDocument42 pages18.fibrinolytic (Thrombolytic) AgentsAstha ShresthaNo ratings yet
- Alteplase PharmacologyDocument24 pagesAlteplase Pharmacologynk999999No ratings yet
- (Printed) Pass Medicine Notes - Clinical Pharmacology & Toxicology (Edited)Document53 pages(Printed) Pass Medicine Notes - Clinical Pharmacology & Toxicology (Edited)Joanne HoNo ratings yet
- Anti-Neoplastic Agents 1Document76 pagesAnti-Neoplastic Agents 1Soubia AamirNo ratings yet
- FIBRINOLYTICS, ANTIPLATELETS AND ANTIFIBRINOLYTICSDocument46 pagesFIBRINOLYTICS, ANTIPLATELETS AND ANTIFIBRINOLYTICSBidyut BanerjeeNo ratings yet
- 4 THROMBOLYTIC DRUGS by DR Azmat AliDocument90 pages4 THROMBOLYTIC DRUGS by DR Azmat AliAhmed YTNo ratings yet
- Immunosuppressive DrugsDocument40 pagesImmunosuppressive DrugsTamjid HossainNo ratings yet
- 11-THROMBOLYTIC Drugs-Ishfaq 2016Document34 pages11-THROMBOLYTIC Drugs-Ishfaq 2016Eni Purwaeni100% (2)
- ReportDocument3 pagesReportShams BlitzerNo ratings yet
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Update JW Cheng DdiDocument9 pagesUpdate JW Cheng DdiauliaNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Protease Inhibitors: Assignment OnDocument6 pagesProtease Inhibitors: Assignment OnVinod Kumar0% (1)
- Anti-Cancer DrugsDocument78 pagesAnti-Cancer DrugsLaghari Jamil100% (1)
- Hemostan LineInsert - Asean 2010Document2 pagesHemostan LineInsert - Asean 2010Maybs Palec Pamplona-ParreñoNo ratings yet
- Anticancer DrugsDocument15 pagesAnticancer DrugsArfia Chowdhury Arifa100% (3)
- StreptokinaseDocument8 pagesStreptokinaseemman_abzNo ratings yet
- Anticancer DrugDocument29 pagesAnticancer DrugAnjana PaudelNo ratings yet
- Effects of The Proton Pump Inhibitor Lansoprazole On The Pharmacokinetics and Pharmacodynamics ofDocument11 pagesEffects of The Proton Pump Inhibitor Lansoprazole On The Pharmacokinetics and Pharmacodynamics ofLuciana OliveiraNo ratings yet
- Myrin P ForteDocument3 pagesMyrin P ForteJohn Zedric Villanueva ArciagaNo ratings yet
- Thrombolytics & Anti Platelet DrugsDocument38 pagesThrombolytics & Anti Platelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Lab Assessment of FibirnolysisDocument8 pagesLab Assessment of FibirnolysisValdez Francis ZaccheauNo ratings yet
- Biotransformasi: Fase I, Fase II, Enzim Terlibat, Sitokrom P450, dan Faktor GenetikDocument38 pagesBiotransformasi: Fase I, Fase II, Enzim Terlibat, Sitokrom P450, dan Faktor GenetikTheresia VirginiaNo ratings yet
- Thrombolytic Agents: Benedict R. Lucchesi, M.D., Ph.D. Department of Pharmacology University of Michigan Medical SchoolDocument15 pagesThrombolytic Agents: Benedict R. Lucchesi, M.D., Ph.D. Department of Pharmacology University of Michigan Medical Schoolnaga chaitanya100% (1)
- Drug StudyDocument2 pagesDrug StudymatthewchadNo ratings yet
- Abstract 1Document3 pagesAbstract 1Sead RizvanovićNo ratings yet
- Thrombolytic TherapyDocument13 pagesThrombolytic TherapyAnusha AkhilNo ratings yet
- Agent Used in Disorder in CoagulationDocument34 pagesAgent Used in Disorder in CoagulationClinton Franda Markus SitanggangNo ratings yet
- Tretinoin Monograph 1feb2014Document6 pagesTretinoin Monograph 1feb2014Milad RostamiNo ratings yet
- Strep To KinDocument21 pagesStrep To Kinfadi kimyaNo ratings yet
- Thrombolytics, Anticoags, Antiplatelets PDFDocument21 pagesThrombolytics, Anticoags, Antiplatelets PDFrachelkdoNo ratings yet
- The Fibrinolytic System: Mysteries and Opportunities: Robert L. Medcalf, Charithani B. KeragalaDocument7 pagesThe Fibrinolytic System: Mysteries and Opportunities: Robert L. Medcalf, Charithani B. KeragalaRicardo EscNo ratings yet
- Penelitian GlyserizinDocument9 pagesPenelitian GlyserizinNovita ApramadhaNo ratings yet
- Effect of Clopidogrel On The Steady-State Pharmacokinetics of FluvastatinDocument8 pagesEffect of Clopidogrel On The Steady-State Pharmacokinetics of FluvastatinLuciana OliveiraNo ratings yet
- Anticancer DrugsDocument26 pagesAnticancer DrugsNeha Chugh100% (1)
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- Cdk2 Activation by Cyclin Binding and PhosphorylationDocument3 pagesCdk2 Activation by Cyclin Binding and PhosphorylationMUHAMMAD ARIFFUDINNo ratings yet
- Activity 11 MetabolismDocument6 pagesActivity 11 MetabolismdavenNo ratings yet
- Med Chem Tutoring Session 2Document34 pagesMed Chem Tutoring Session 2Morrigan DearmanNo ratings yet
- 12-2023 Questions - MergedDocument162 pages12-2023 Questions - MergedAANo ratings yet
- TDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Document11 pagesTDM: Cyclosporin: Course: Advanced Clinical Pharmacy Corse No 711-T Course Incharge: Saima Saleem (Assistant Professor)Samra KhanNo ratings yet
- Topic HemostasisDocument10 pagesTopic HemostasisFatemeh EshaghizadehNo ratings yet
- Drug Interaction-SibyDocument93 pagesDrug Interaction-SibyAswin DamodaranNo ratings yet
- Jurnal Reading InternaDocument10 pagesJurnal Reading InternaKrishnaNo ratings yet
- ThalassemiaDocument33 pagesThalassemiaRyan ArcuenoNo ratings yet
- Drugs Affecting Blood Cloting 2019Document39 pagesDrugs Affecting Blood Cloting 2019Mutiara RizkiNo ratings yet
- Antifibrinolytic Drugs and Perioperative Hemostasis Authors: Slaughter, Thomas F. Greenberg, Charles S.Document5 pagesAntifibrinolytic Drugs and Perioperative Hemostasis Authors: Slaughter, Thomas F. Greenberg, Charles S.ionaiobidzeNo ratings yet
- NilotinibDocument2 pagesNilotinibBigBoostingNo ratings yet
- p450 LiquinyangDocument4 pagesp450 LiquinyangThoriqotil Haqqul MauludiyahNo ratings yet
- Yang 2018Document16 pagesYang 2018Sadia qaziNo ratings yet
- Drug TransplantationDocument36 pagesDrug Transplantationsajad abasewNo ratings yet
- Adult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Document3 pagesAdult: IV Nosocomial Pneumonia Empiric Therapy For Febrile Neutropenic Patients 4.5Chris Denver BancaleNo ratings yet
- Drug StudyDocument6 pagesDrug StudyMarielle Denise Tagtag BugtongNo ratings yet
- Avelumab Merkel Cell Carcinoma Protocol V1.1Document6 pagesAvelumab Merkel Cell Carcinoma Protocol V1.1Vlad CroitoruNo ratings yet
- Cellular Endocrinology in Health and DiseaseFrom EverandCellular Endocrinology in Health and DiseaseAlfredo Ulloa-AguirreNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Hobfoll Et Al., 2018 PDFDocument28 pagesHobfoll Et Al., 2018 PDFQundeel HaiderNo ratings yet
- The Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipDocument15 pagesThe Relationship Between Challenge and Hindrance Stressors and Emotional Exhaustion: The Moderating Role of Perceived Servant LeadershipmehakNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Michel On 2010Document33 pagesMichel On 2010Tawsif HasanNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Journal of Cleaner Production: Marco Formentini, Paolo TaticchiDocument14 pagesJournal of Cleaner Production: Marco Formentini, Paolo TaticchiJuan AlmeydaNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Relationship Between Corporate Governance, Corporate Sustainability and Financial PerformanceDocument21 pagesRelationship Between Corporate Governance, Corporate Sustainability and Financial PerformancemehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
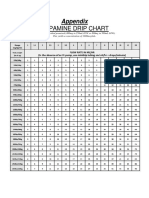
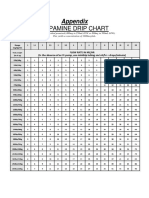
- Dopamine Drip Chart AppendixDocument1 pageDopamine Drip Chart AppendixmehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Current Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDDocument9 pagesCurrent Management of Hepatocellular Carcinoma: Ana Maria Crissien, MD, and Catherine Frenette, MDmehakNo ratings yet
- Guias Del Uso de Albumina e IgGDocument19 pagesGuias Del Uso de Albumina e IgGRonny Muñoz AcuñaNo ratings yet
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- NOAC Comparison ChartDocument1 pageNOAC Comparison ChartrsouzaNo ratings yet
- Jurnal ICH 2008Document6 pagesJurnal ICH 2008Yusuf Agung NugrohoNo ratings yet
- Articol 8Document11 pagesArticol 8Cosmin GabrielNo ratings yet
- Apostila R2Document469 pagesApostila R2Lucas TheotonioNo ratings yet
- Primary Sample Collection Manual GD-QSPMDocument51 pagesPrimary Sample Collection Manual GD-QSPMLalit Surykant ChavanNo ratings yet
- HIS1-K38 Obat-Obat Pada Gangguan Koagulasi (Antikoagulan)Document40 pagesHIS1-K38 Obat-Obat Pada Gangguan Koagulasi (Antikoagulan)Ega FlorenceNo ratings yet
- Caldeira 2018Document6 pagesCaldeira 2018Engels Yeltsin Ponce GonzalesNo ratings yet
- Pharmacology Review Drugs That Alter Blood Coagulation PDFDocument6 pagesPharmacology Review Drugs That Alter Blood Coagulation PDFyouyayuNo ratings yet
- Treatment Considerations, and Nursing Implications: Cardiovascular Disease and HIV: PathophysiologyDocument12 pagesTreatment Considerations, and Nursing Implications: Cardiovascular Disease and HIV: PathophysiologyRicardo Costa da SilvaNo ratings yet
- Ghid ERHA Privitor NOAK 2018 PDFDocument64 pagesGhid ERHA Privitor NOAK 2018 PDFSolaris CorbutNo ratings yet
- Rivaroxaban For Stroke Prevention Journal FadelDocument17 pagesRivaroxaban For Stroke Prevention Journal Fadelahmadzia btrNo ratings yet
- Vasodilator and Anticoagulant Agents SummaryDocument23 pagesVasodilator and Anticoagulant Agents Summarymonyet65No ratings yet
- Periprocedural Anticoagulation Guidelines - UKDocument14 pagesPeriprocedural Anticoagulation Guidelines - UKjoshNo ratings yet
- Ensaio Clínico - Rivaroxaban Vs Warfarin in High-Risk Patients WithDocument7 pagesEnsaio Clínico - Rivaroxaban Vs Warfarin in High-Risk Patients WithesdrasNo ratings yet
- Surgical Care Improvement Project JCIDocument50 pagesSurgical Care Improvement Project JCIKania FitrianiNo ratings yet
- Clark Blue Book CARDIODocument181 pagesClark Blue Book CARDIOChristian SunurNo ratings yet
- Sdcep Management of Dental Patients Taking Anticoagulants or Antiplatelet Drugs 2nd EditionDocument58 pagesSdcep Management of Dental Patients Taking Anticoagulants or Antiplatelet Drugs 2nd EditionMeryem LahlouNo ratings yet
- NOAC Trong Rung NhĩDocument23 pagesNOAC Trong Rung NhĩToan ngoNo ratings yet
- American College of Gastroenterology Canadian Association of GastroenterologyDocument18 pagesAmerican College of Gastroenterology Canadian Association of GastroenterologyGW GeistNo ratings yet
- Venous Thromboembolism (VTE) - McMaster Pathophysiology ReviewDocument9 pagesVenous Thromboembolism (VTE) - McMaster Pathophysiology ReviewFadiyah UlfahNo ratings yet
- Perioperative Anticoagulation Bridging Guideline PostedDocument6 pagesPerioperative Anticoagulation Bridging Guideline PostedNuc Alexandru100% (1)
- XareltoDocument9 pagesXareltoapi-309201467No ratings yet
- Guideline For Patients Receiving Apixaban (Eliquis) Requiring Emergency Surgery or Treatment For HaemorrhageDocument7 pagesGuideline For Patients Receiving Apixaban (Eliquis) Requiring Emergency Surgery or Treatment For HaemorrhageAndresPimentelAlvarezNo ratings yet
- Switching To-From AnticoagulantsDocument8 pagesSwitching To-From AnticoagulantsAlex AlxNo ratings yet
- 08) Acmtac-Protocol-2019-Revised - 1Document86 pages08) Acmtac-Protocol-2019-Revised - 1Teh NuraqilahNo ratings yet
- Neuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDateDocument25 pagesNeuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDatemago1961100% (1)
- Research 31 PDFDocument68 pagesResearch 31 PDFRamu SanjappagariNo ratings yet
- Anticoagulation PharmacologyDocument36 pagesAnticoagulation PharmacologyaymenNo ratings yet