You might also like
- BoswellOlson BuchananLePine2004JVBStressDocument18 pagesBoswellOlson BuchananLePine2004JVBStressmehakNo ratings yet
- A Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchDocument12 pagesA Review of The Challenge-Hindrance Stress Model: Recent Advances, Expanded Paradigms, and Recommendations For Future ResearchmehakNo ratings yet
- Job Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementDocument12 pagesJob Satisfaction, Organizational Commitment and Job Involvement: The Mediating Role of Job InvolvementmehakNo ratings yet
- A Review Corporate Governance and SustainabilityDocument11 pagesA Review Corporate Governance and SustainabilitymehakNo ratings yet
- Impact of Corporate Governance On Corporate Sustainable GrowthDocument18 pagesImpact of Corporate Governance On Corporate Sustainable GrowthmehakNo ratings yet
- Corporate Governance Integration With Sustainability: A Systematic Literature ReviewDocument15 pagesCorporate Governance Integration With Sustainability: A Systematic Literature ReviewmehakNo ratings yet
- Ijbel22 204Document9 pagesIjbel22 204mehakNo ratings yet
- This Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCDocument8 pagesThis Content Downloaded From 202.43.95.25 On Tue, 05 Oct 2021 01:35:52 UTCmehakNo ratings yet
- Governance and SustainabilityDocument17 pagesGovernance and SustainabilitymehakNo ratings yet
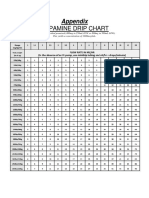
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
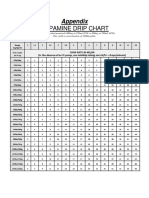
- Dopamine Drip ChartDocument1 pageDopamine Drip ChartmehakNo ratings yet
- The Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchDocument30 pagesThe Corporate Governance of Environmental Sustainability: A Review and Proposal For More Integrated ResearchmehakNo ratings yet
- Anak - Kasus 7 - Kelompok 7Document48 pagesAnak - Kasus 7 - Kelompok 7mehakNo ratings yet
- The Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapyDocument9 pagesThe Correlation of Structural and Binding Affinity of Insulin Analog To The Onset of Action For Diabetic TherapymehakNo ratings yet
- Zhou2019 Article InsulinDegludecANovelUltra-LonDocument18 pagesZhou2019 Article InsulinDegludecANovelUltra-LonmehakNo ratings yet
- Kementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggiDocument11 pagesKementerian Pendidikan, Kebudayaan Riset Dan Teknologi: Direktorat Jenderal Pendidikan TinggimehakNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- He Pat EctomyDocument4 pagesHe Pat Ectomysharjil chaudhryNo ratings yet
- Date Year Hs Code Product QuantityunitDocument45 pagesDate Year Hs Code Product QuantityunitProschool HyderabadNo ratings yet
- Acute Cholecystitis: Lim Liang YikDocument68 pagesAcute Cholecystitis: Lim Liang YikLim Liang YikNo ratings yet
- Choledochal CystDocument16 pagesCholedochal CystNico HernándezNo ratings yet
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- LFT LalpathDocument2 pagesLFT Lalpathmoyic39272No ratings yet
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocument47 pagesJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNo ratings yet
- MedicamenteDocument3 pagesMedicamentecraciun monicaNo ratings yet
- Clinical Characteristics, Treatment, and Prognosis of Patients With Obstructive Jaundice in Tertiary Care Facilities: A Prospective StudyDocument4 pagesClinical Characteristics, Treatment, and Prognosis of Patients With Obstructive Jaundice in Tertiary Care Facilities: A Prospective Studyrifa iNo ratings yet
- Asuhan Keperawatan Pada Pasien Chirosis HepatisDocument48 pagesAsuhan Keperawatan Pada Pasien Chirosis HepatisRheni WidyaNo ratings yet
- Neonatal JaundiceDocument2 pagesNeonatal JaundiceyahyuNo ratings yet
- Mirizzi Syndrome-Rare Cause of Major Biliary Complications. Case ReportDocument3 pagesMirizzi Syndrome-Rare Cause of Major Biliary Complications. Case ReportWelviraHandayaniNo ratings yet
- Jaundice: Dr. Soegiarto Gani, SPPDDocument24 pagesJaundice: Dr. Soegiarto Gani, SPPDmirwan bakriNo ratings yet
- Gallbladder - Gallstones and SurgeryDocument4 pagesGallbladder - Gallstones and SurgeryVinod MeenaNo ratings yet
- Curs 15v-2018hDocument96 pagesCurs 15v-2018hMirceaDraghiciNo ratings yet
- A Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFDocument7 pagesA Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFHemin HassanNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaMel DaNo ratings yet
- 61Document205 pages61Carlos HernándezNo ratings yet
- Liver Structure Funciton QnsDocument4 pagesLiver Structure Funciton QnsNoora AttariNo ratings yet
- Liver Function Reviewer Cc2Document7 pagesLiver Function Reviewer Cc2Leo NoquilNo ratings yet
- Nicolás Alberto Cely Aldana Interno Fujnc Agosto-2020Document62 pagesNicolás Alberto Cely Aldana Interno Fujnc Agosto-2020nicolasNo ratings yet
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
- Child-Pugh Score & MELDDocument3 pagesChild-Pugh Score & MELDChaterine GraceNo ratings yet
- Cholecystitis Pathophysiology Schematic DiagramDocument2 pagesCholecystitis Pathophysiology Schematic DiagramChristyl CalizoNo ratings yet
- Dr. Brendalyn A. Gallebo Department of Histopath and LaboratoriesDocument216 pagesDr. Brendalyn A. Gallebo Department of Histopath and LaboratoriesFelyne Angelique C. GanoticeNo ratings yet
- Obstructive JaundiceDocument15 pagesObstructive JaundiceUjas Patel100% (4)
- Hepatobiliary System-Anatomy & PhysiologyDocument49 pagesHepatobiliary System-Anatomy & PhysiologyDeshi SportsNo ratings yet
- SinonimDocument3 pagesSinonimindah indahNo ratings yet
- Chapter - 2 - C - II Liver CirrhosisDocument39 pagesChapter - 2 - C - II Liver CirrhosisEmmaNo ratings yet
- Noninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDateDocument35 pagesNoninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDatepopasorinemilianNo ratings yet