You might also like
- Arthroplasty JournalDocument3 pagesArthroplasty Journallina yohanes100% (1)
- Psychoactive Substances and Paranormal Phenomena: A Comprehensive ReviewDocument60 pagesPsychoactive Substances and Paranormal Phenomena: A Comprehensive ReviewDavid LukeNo ratings yet
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoNo ratings yet
- Renvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1Document9 pagesRenvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1FelipeOyarceSalazarNo ratings yet
- Chiropractic PDFDocument20 pagesChiropractic PDFAlexandru Cristian StanciuNo ratings yet
- Quarter 2 - Module 3 - Earth and Life ScienceDocument6 pagesQuarter 2 - Module 3 - Earth and Life ScienceKristine AlcordoNo ratings yet
- Frog DissectionDocument4 pagesFrog DissectionRouse Leanne NicolasNo ratings yet
- PAL: Histology Connective Tissue Quiz Question 1Document20 pagesPAL: Histology Connective Tissue Quiz Question 1muryum100% (1)
- Peri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsDocument9 pagesPeri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsFrancisca Cardenas OñateNo ratings yet
- Dapus RaddDocument20 pagesDapus RaddNur Liza SeptianiNo ratings yet
- Editorial: Decisions and Antibiotics Use: More Questions and Some AnswersDocument3 pagesEditorial: Decisions and Antibiotics Use: More Questions and Some AnswersTommy Leon SilvaNo ratings yet
- Peeters, Putzeys, Thorrez - Unknown - 2019 - Current Insights in The Application of Bone Grafts For Local Antibiotic Delivery in Bone ReDocument9 pagesPeeters, Putzeys, Thorrez - Unknown - 2019 - Current Insights in The Application of Bone Grafts For Local Antibiotic Delivery in Bone ReLievenNo ratings yet
- BursitisDocument9 pagesBursitisRauLTMZNo ratings yet
- Salter EnglishDocument3 pagesSalter EnglishAndyno SanjayaNo ratings yet
- The Management of Acute Bone and Joint Infection in ChildhoodDocument15 pagesThe Management of Acute Bone and Joint Infection in ChildhoodTalia LizardiNo ratings yet
- Journal of Negative Results in BiomedicineDocument5 pagesJournal of Negative Results in Biomedicinedef_10No ratings yet
- Antibiotic BeadsDocument5 pagesAntibiotic Beadsratnav_ratanNo ratings yet
- Biofilm in OtorhinolaryngologyDocument10 pagesBiofilm in OtorhinolaryngologyMohammed SahibNo ratings yet
- Current Concept of Abdominal Sepsis: WSES Position Paper: World Journal of Emergency Surgery March 2014Document17 pagesCurrent Concept of Abdominal Sepsis: WSES Position Paper: World Journal of Emergency Surgery March 2014Muhammad Hisyam AjimulyaNo ratings yet
- Prophylactic Antibiotics in Hip and Knee ArthroplastyDocument11 pagesProphylactic Antibiotics in Hip and Knee ArthroplastySara Aly YoussefNo ratings yet
- Antibiotic Prophylaxis For Orthognathic SurgeryDocument5 pagesAntibiotic Prophylaxis For Orthognathic SurgeryNatalia AssolariNo ratings yet
- Antibiotic TreatmentDocument25 pagesAntibiotic TreatmentNailil khusnaNo ratings yet
- AAE Position StatementDocument5 pagesAAE Position StatementCarlos San MartinNo ratings yet
- Case DefinitionsDocument9 pagesCase DefinitionsCarlos Armijos SNo ratings yet
- Management and Follow-Up Results of Salivary Fistulas TreatedDocument6 pagesManagement and Follow-Up Results of Salivary Fistulas Treatedluis castroNo ratings yet
- 1.1 Background: It Is Commonly Found That TheDocument14 pages1.1 Background: It Is Commonly Found That ThetorkNo ratings yet
- Treating Osteomyelitis: Antibiotics and Surgery: BackgroundDocument11 pagesTreating Osteomyelitis: Antibiotics and Surgery: BackgroundCarolina MachadoNo ratings yet
- International Journal of Infectious DiseasesDocument7 pagesInternational Journal of Infectious DiseasesYuda BeduNo ratings yet
- s13104 016 2245 6Document8 pagess13104 016 2245 6DeiGNo ratings yet
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioDocument7 pagesThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniNo ratings yet
- Aae Systemic AntibioticsDocument8 pagesAae Systemic AntibioticsIulia CiobanuNo ratings yet
- Bilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportDocument4 pagesBilateral Acute Tibial Osteomyelitis in A Patient Without An Underlying Disease: A Case ReportIfal JakNo ratings yet
- Garlic Extract in Prosthesis-Related Infections: A Literature ReviewDocument10 pagesGarlic Extract in Prosthesis-Related Infections: A Literature ReviewnacenkNo ratings yet
- Antibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.HDocument2 pagesAntibiotics For Abdominal Sepsis: Richard P. Wenzel, M.D., and Michael B. Edmond, M.D., M.P.Hchebonk13No ratings yet
- Abdominal Sepsis.15Document8 pagesAbdominal Sepsis.15Dario Xavier Achachi MelendezNo ratings yet
- Influence of The Intestinal Microbiome On Anastomotic Healing in The Colon and RectumDocument25 pagesInfluence of The Intestinal Microbiome On Anastomotic Healing in The Colon and RectumDumitru RadulescuNo ratings yet
- Antibiotics 13 00289Document17 pagesAntibiotics 13 00289Jeniffer VillamilNo ratings yet
- The Characteristics of Biofilms in Peri-Implant DiseaseDocument11 pagesThe Characteristics of Biofilms in Peri-Implant DiseaseSheilaNo ratings yet
- Golden Hour CCM Arthur Van Zanten IC1Document3 pagesGolden Hour CCM Arthur Van Zanten IC1Sara NicholsNo ratings yet
- TRI - Immunophasic Therapy: A Future LandscapeDocument4 pagesTRI - Immunophasic Therapy: A Future LandscapeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Is Bleeding On Probing A Differential Diagnosis Between Periimplant Health and Disease?Document5 pagesIs Bleeding On Probing A Differential Diagnosis Between Periimplant Health and Disease?Tonya GoldenNo ratings yet
- Journal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithDocument14 pagesJournal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithShakeel AhmedNo ratings yet
- Researchtopic PEDScaringpaperDocument6 pagesResearchtopic PEDScaringpaperПАПА ДЖЕЙКNo ratings yet
- Bone Infections: OsteomyelitisDocument6 pagesBone Infections: OsteomyelitisMarius Clifford BilledoNo ratings yet
- Malleolar Fractures: Surgical Site Infection and Its Risk FactorsDocument18 pagesMalleolar Fractures: Surgical Site Infection and Its Risk FactorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Case Report of A Tongue Ulcer Presented As The First Sign of Occult TuberculosisDocument5 pagesA Case Report of A Tongue Ulcer Presented As The First Sign of Occult TuberculosisSasa AprilaNo ratings yet
- 35journal of Periodontology - 2018 - Renvert - Peri Implant Health Peri Implant Mucositis and Peri Implantitis CaseDocument9 pages35journal of Periodontology - 2018 - Renvert - Peri Implant Health Peri Implant Mucositis and Peri Implantitis CaseMax Flores RuizNo ratings yet
- FullDocument9 pagesFullهادي تركي شنبارةNo ratings yet
- Fphar 10 01137Document8 pagesFphar 10 01137Kajelcha FikaduNo ratings yet
- Pathogenesis and Management of Fracture-Related InfectionDocument7 pagesPathogenesis and Management of Fracture-Related InfectionJeremi SetiawanNo ratings yet
- Treatment Strategy For Frozen ShoulderDocument9 pagesTreatment Strategy For Frozen ShoulderDiah Rindayani HasbiNo ratings yet
- Biomedicines 12 00715Document21 pagesBiomedicines 12 00715jamel-shamsNo ratings yet
- Antibiotics in Dentistry - 2013Document4 pagesAntibiotics in Dentistry - 2013Delia GardeaNo ratings yet
- Med Surg Pico-2Document11 pagesMed Surg Pico-2Jason Kennedy100% (1)
- Gels 08 00163Document10 pagesGels 08 00163Andreea BarbuNo ratings yet
- Jenkinson, Et Al (2014)Document7 pagesJenkinson, Et Al (2014)rachid hattabNo ratings yet
- A. Introduction OsteomyelitisDocument10 pagesA. Introduction OsteomyelitisMa. Gina DerlaNo ratings yet
- Animal Models of Mucositis Implications For TherapDocument9 pagesAnimal Models of Mucositis Implications For TherapÁgnesJanovszkyNo ratings yet
- Latent Infection of Low-Virulence Anaerobic Bacteria in Degenerated Lumbar Intervertebral DiscsDocument5 pagesLatent Infection of Low-Virulence Anaerobic Bacteria in Degenerated Lumbar Intervertebral Discsvg04No ratings yet
- Antibiotic Resistance Thesis StatementDocument6 pagesAntibiotic Resistance Thesis Statementkatelogebellevue100% (2)
- Antibiotics in Orthopedic InfectionsDocument3 pagesAntibiotics in Orthopedic InfectionsDania ZaidNo ratings yet
- Peri-Implant Mucositis and Peri-Implantitis: A Current Understanding of Their Diagnoses and Clinical ImplicationsDocument8 pagesPeri-Implant Mucositis and Peri-Implantitis: A Current Understanding of Their Diagnoses and Clinical Implicationsjabp1691No ratings yet
- Postopertive Spinal Implant InfectionDocument8 pagesPostopertive Spinal Implant InfectionVu AnNo ratings yet
- Treatment of Non-infectious UveitisFrom EverandTreatment of Non-infectious UveitisPhoebe LinNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
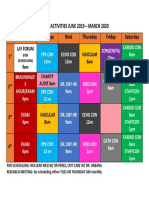
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- IungDocument8 pagesIungReda SoNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoNo ratings yet
- Forrajes Tropicales PDFDocument165 pagesForrajes Tropicales PDFBrigith Briceño RomeroNo ratings yet
- Nepal Health Professional Council: Syllabus For Professional Licensing Examination of Grade A-Diagnostic Health LabDocument10 pagesNepal Health Professional Council: Syllabus For Professional Licensing Examination of Grade A-Diagnostic Health LabBhageshwar ChaudharyNo ratings yet
- NURS 04 RLE - Sterile Field and Wound DressingDocument3 pagesNURS 04 RLE - Sterile Field and Wound DressingayresNo ratings yet
- Use of Genetic Algorithm To Resolve The Problem of Finite State Machine ConstructionDocument18 pagesUse of Genetic Algorithm To Resolve The Problem of Finite State Machine ConstructionDevendra SharmaNo ratings yet
- Phytochemical and Pharmacological Profile of Ipomoea AquaticaDocument13 pagesPhytochemical and Pharmacological Profile of Ipomoea AquaticaMega Silvia HasugianNo ratings yet
- LocomotionDocument13 pagesLocomotionPrakhar SrivastavaNo ratings yet
- Bleach JumpChainDocument31 pagesBleach JumpChainAlessioNo ratings yet
- Conducting and Interpreting Fish Telemetry Studies: Considerations For Researchers and Resource ManagersDocument32 pagesConducting and Interpreting Fish Telemetry Studies: Considerations For Researchers and Resource ManagersCacique SamuraiNo ratings yet
- Lesson 3 Nervous SystemDocument11 pagesLesson 3 Nervous SystemMARY JANE ANGELICA SEVANo ratings yet
- Descola e Palsson - 1996 - IntroductionDocument12 pagesDescola e Palsson - 1996 - IntroductionUtsch FabianoNo ratings yet
- MyGo Pro Brochure FinalDocument7 pagesMyGo Pro Brochure FinalDũng NguyễnNo ratings yet
- Altro - Vitamina C PureWay - C - WEBDocument2 pagesAltro - Vitamina C PureWay - C - WEBluigi cardanoNo ratings yet
- Born Barry 2010Document18 pagesBorn Barry 2010Vicente ReisNo ratings yet
- Yasmin Moez ResumeDocument1 pageYasmin Moez Resumeapi-490664639No ratings yet
- 4 Years Bachelor of Science (B.SC.) Programme Micro-Syllabus of B.Sc. First Year ZoologyDocument12 pages4 Years Bachelor of Science (B.SC.) Programme Micro-Syllabus of B.Sc. First Year ZoologyAnwita JhaNo ratings yet
- Introduction To Plant Pathology-Lecture 2Document22 pagesIntroduction To Plant Pathology-Lecture 2Oluwapelumi Adesola AdeyemiNo ratings yet
- Ficus Microcarpa HawaiiDocument2 pagesFicus Microcarpa Hawaiiloganhady8No ratings yet
- Graft Versus Host Disease..Document2 pagesGraft Versus Host Disease..Sakawath HosainNo ratings yet
- Rashevsky - Topology and LifeDocument32 pagesRashevsky - Topology and LifeEva GoaforNo ratings yet
- ADIL BSN - 1C 11. Manual Reproductive SystemDocument4 pagesADIL BSN - 1C 11. Manual Reproductive SystemReiko SakaeNo ratings yet
- Fema FlavorDocument36 pagesFema FlavorEmilio PalomaresNo ratings yet
- Enzyme Histochemistry A Laboratory Manual by Prof DR Zdeněk Lojda PDFDocument349 pagesEnzyme Histochemistry A Laboratory Manual by Prof DR Zdeněk Lojda PDFSwathi JNo ratings yet
- Ration Formulation MethodDocument2 pagesRation Formulation MethodHobi JungNo ratings yet
- This That/ These Those: MWW.W MammDocument2 pagesThis That/ These Those: MWW.W MammJosue SanNo ratings yet
- 1 s2.0 S2001037020303937 MainDocument15 pages1 s2.0 S2001037020303937 MainRaja KumarNo ratings yet