You might also like
- How To Warm Up On Sunday Morning WorkbookDocument9 pagesHow To Warm Up On Sunday Morning WorkbookErin Doramis RomanNo ratings yet
- Electrophysiology of LarynxDocument12 pagesElectrophysiology of LarynxNehasish SahuNo ratings yet
- ShiatsuDocument17 pagesShiatsuapi-275305557No ratings yet
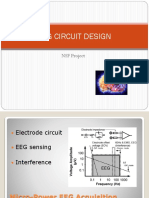
- Eeg Circuit Design: NSF ProjectDocument136 pagesEeg Circuit Design: NSF Projectrhycardo5902No ratings yet
- Sickle Cell AnemiaDocument20 pagesSickle Cell AnemiaAnastasiafynn100% (1)
- Muscular System Quiz 01 - Attempt ReviewDocument13 pagesMuscular System Quiz 01 - Attempt ReviewPsalm Jirehmae SantosNo ratings yet
- EC2021-Medical Electronics Notes For All Five UnitsDocument147 pagesEC2021-Medical Electronics Notes For All Five UnitsJason Jackson100% (1)
- Ecg Eeg EmgDocument16 pagesEcg Eeg EmgNeha100% (1)
- Neurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindFrom EverandNeurofeedback - The Neurofeedback Book for Patients and Therapists : A Symphony of the MindNo ratings yet
- The Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)From EverandThe Physics and Technology of Diagnostic Ultrasound: Study Guide (Second Edition)No ratings yet
- Coronary Circulation FDocument36 pagesCoronary Circulation FjefferyNo ratings yet
- 31 Plant Hormones-SDocument6 pages31 Plant Hormones-SLeo Ding0% (1)
- Eeg Circuit Design: NSF ProjectDocument136 pagesEeg Circuit Design: NSF ProjectJesus Peña100% (2)
- Fundamentals of Eeg MeasurementDocument11 pagesFundamentals of Eeg Measurementfiziomar8100% (2)
- Human Longevity Project Vitality Experience Guidebook 2Document42 pagesHuman Longevity Project Vitality Experience Guidebook 2Britt LangNo ratings yet
- Clinical Neurophysiology and Electroencephalography: Jong Woo Lee, MD, PHD, and Shahram Khoshbin, MDDocument9 pagesClinical Neurophysiology and Electroencephalography: Jong Woo Lee, MD, PHD, and Shahram Khoshbin, MDEmilio SanchezNo ratings yet
- Clinical Electro Physiological TestingDocument22 pagesClinical Electro Physiological TestingPaul VkNo ratings yet
- AcupuncturePointCompendium2014 PDFDocument269 pagesAcupuncturePointCompendium2014 PDFlinecurNo ratings yet
- World University of Bangladesh: Report On Radiography of The Brain (EEG)Document10 pagesWorld University of Bangladesh: Report On Radiography of The Brain (EEG)EmonNo ratings yet
- SSEPDocument12 pagesSSEPahippo100% (1)
- (Electroencephalogram) An Introduction: By: Muhammad Farooq Supervisors: Dr. Aamir Saeed Malik Dr. Mohd Zuki Bin YousaffDocument31 pages(Electroencephalogram) An Introduction: By: Muhammad Farooq Supervisors: Dr. Aamir Saeed Malik Dr. Mohd Zuki Bin YousafffarooqespnNo ratings yet
- Nerve Conduction StudiesDocument210 pagesNerve Conduction Studieshm3398100% (3)
- Brain Oscillations, Synchrony and Plasticity: Basic Principles and Application to Auditory-Related DisordersFrom EverandBrain Oscillations, Synchrony and Plasticity: Basic Principles and Application to Auditory-Related DisordersNo ratings yet
- United Neurodiagnostic Professionals of America - EMG and Evoked Potentials in The Operating Room During Spinal SurgeryDocument12 pagesUnited Neurodiagnostic Professionals of America - EMG and Evoked Potentials in The Operating Room During Spinal SurgeryShauki AliNo ratings yet
- Sherwood 1981Document7 pagesSherwood 1981DANIEL ARTEAGA MENDOZANo ratings yet
- Sistem Saraf Pusat (Central Nervous System)Document23 pagesSistem Saraf Pusat (Central Nervous System)Ruspata BhyantariNo ratings yet
- Emg Conceptos - Nerve Conduction StudiesDocument23 pagesEmg Conceptos - Nerve Conduction StudiesDeborah SalinasNo ratings yet
- Nerve Conduction Study-3Document8 pagesNerve Conduction Study-3thestaffforpediatricptNo ratings yet
- Medscape Neurophysiological MonitoringDocument10 pagesMedscape Neurophysiological MonitoringTomagratchNo ratings yet
- Presentación de ArtículoDocument12 pagesPresentación de ArtículoSofia Josefa Beatriz Espinoza RosasNo ratings yet
- Estudios de Conduccion NerviosaDocument8 pagesEstudios de Conduccion NerviosaSoledad CáceresNo ratings yet
- Portable EEG Signal Acquisition SystemDocument8 pagesPortable EEG Signal Acquisition SystemcalsomoNo ratings yet
- Bucht Hal 1955Document17 pagesBucht Hal 1955It's RohanNo ratings yet
- Laryngeal ElectromyographyDocument21 pagesLaryngeal Electromyographyapi-19500641No ratings yet
- EMG Lead PlacementDocument14 pagesEMG Lead PlacementalanNo ratings yet
- ON Electroencephalogram (EEG) Done By: Biomedical Department B.E 2 /4 SemDocument11 pagesON Electroencephalogram (EEG) Done By: Biomedical Department B.E 2 /4 SemSai TejaNo ratings yet
- EEG (ElectroEncephaloGraph)Document47 pagesEEG (ElectroEncephaloGraph)Dhvij KmlNo ratings yet
- 2003 - A Study of The Dynamic Interactions Between Sleep EEG and Heart Rate Variability in Healthy Young MenDocument10 pages2003 - A Study of The Dynamic Interactions Between Sleep EEG and Heart Rate Variability in Healthy Young MenVeronica JanethNo ratings yet
- Orthodromic Vs AntidromicDocument9 pagesOrthodromic Vs AntidromicahmedNo ratings yet
- mfd2011 Basis MEEGDocument49 pagesmfd2011 Basis MEEGMichael HabibNo ratings yet
- Lab 2Document6 pagesLab 2api-272723910No ratings yet
- NCV StudyDocument60 pagesNCV StudyhiralNo ratings yet
- Measurement System:: Signal Processing, ADC and Digital ProcessingDocument1 pageMeasurement System:: Signal Processing, ADC and Digital ProcessingZz_TyranT_zZNo ratings yet
- Medical Applications of DSP: Made By-Digisha Singhal Kinjal Aggrawal 13bec026 13bec054 Guided by - Dr. Mehul NaikDocument28 pagesMedical Applications of DSP: Made By-Digisha Singhal Kinjal Aggrawal 13bec026 13bec054 Guided by - Dr. Mehul NaikRahmatullahNo ratings yet
- 1 s2.0 S1388245700002480 MainDocument4 pages1 s2.0 S1388245700002480 MainMoon PowerNo ratings yet
- What Is Ncs ?Document42 pagesWhat Is Ncs ?rabeyaNo ratings yet
- GoldmanEEG fMRIDocument7 pagesGoldmanEEG fMRIvkumar8282No ratings yet
- TrapecioDocument7 pagesTrapecioEdgardo BivimasNo ratings yet
- ElectroencephalographyDocument14 pagesElectroencephalographykdafloresaNo ratings yet
- Applsci 10 01797 v2Document12 pagesApplsci 10 01797 v2Uagro TicsNo ratings yet
- Eggermont 2019 ABRDocument15 pagesEggermont 2019 ABRSujeet PathakNo ratings yet
- 5 EEG-historiaDocument21 pages5 EEG-historiaRodrigo A.S.No ratings yet
- Period-Amplitude Analysis of Rat Electroencephalogram: Stage and Diurnal Variations and Effects of Suprachiasmatic Nuclei LesionsDocument14 pagesPeriod-Amplitude Analysis of Rat Electroencephalogram: Stage and Diurnal Variations and Effects of Suprachiasmatic Nuclei Lesions1030006No ratings yet
- HE Origin OF IO PotentialsDocument16 pagesHE Origin OF IO PotentialsThiva KaranNo ratings yet
- 1 s2.0 S0165027002003400 MainDocument19 pages1 s2.0 S0165027002003400 MainVaNo ratings yet
- Tech Foundation TrimDocument9 pagesTech Foundation TrimSHFNo ratings yet
- TestsDocument8 pagesTestsNamrathaThalatoti ywSSAmHsULNo ratings yet
- Unit 3Document25 pagesUnit 3senthilNo ratings yet
- Medical Applications of DSP: Made By-Digisha Singhal 13bec026 Kinjal Aggrawal 13bec054 Guided by - Dr. Mehul NaikDocument16 pagesMedical Applications of DSP: Made By-Digisha Singhal 13bec026 Kinjal Aggrawal 13bec054 Guided by - Dr. Mehul NaikPriyank KeniNo ratings yet
- Problem StatementDocument18 pagesProblem StatementvmrekhateNo ratings yet
- Tinku Biswas, Swarup Sarkar, Akash Ku. Bhoi, Surajit BagchiDocument7 pagesTinku Biswas, Swarup Sarkar, Akash Ku. Bhoi, Surajit BagchiInternational Journal of computational Engineering research (IJCER)No ratings yet
- EEG - Biopac Lesson L04Document18 pagesEEG - Biopac Lesson L04Yunyun LiuNo ratings yet
- 5 CM From The Center of The Chest and The Top: Et AlDocument8 pages5 CM From The Center of The Chest and The Top: Et AlsebascastmNo ratings yet
- Biomedical Ktu EceDocument34 pagesBiomedical Ktu EceGreeshma RatheeshNo ratings yet
- Biomedical Engineering Ktu Mod 3Document12 pagesBiomedical Engineering Ktu Mod 3Adheeb Shibu VattasserilNo ratings yet
- Aspectos MetodológicosDocument8 pagesAspectos MetodológicosDaniela AndreottiNo ratings yet
- A Technique For Studying The Greater Auricular Nerve Conduction VelocityDocument3 pagesA Technique For Studying The Greater Auricular Nerve Conduction Velocityfernando gonzalezNo ratings yet
- Continuous Culture in ChemostatDocument6 pagesContinuous Culture in ChemostatBlessy GabaynoNo ratings yet
- 10 Chapter 1Document29 pages10 Chapter 1percepshanNo ratings yet
- Pha PresentationDocument19 pagesPha PresentationidrisqrNo ratings yet
- PG BOTANY Plant Physiology Question Bank CompleteDocument10 pagesPG BOTANY Plant Physiology Question Bank CompleteAbid ShowketNo ratings yet
- Syllabus BSCBOTDocument18 pagesSyllabus BSCBOTJayanta SikdarNo ratings yet
- Full Download Human Memory 2nd Radvansky Test Bank PDF Full ChapterDocument36 pagesFull Download Human Memory 2nd Radvansky Test Bank PDF Full Chaptersugarysestine.fllo5z100% (21)
- Unit 4 Perception and CoordinationDocument86 pagesUnit 4 Perception and CoordinationMaríaNo ratings yet
- Modul Final Biologi Form 4 Fasa 1 2021Document60 pagesModul Final Biologi Form 4 Fasa 1 2021Manmohon Kaur100% (1)
- Gurvinder Kalra,: MD, DPM Psychiatrist Lrh-MhsDocument16 pagesGurvinder Kalra,: MD, DPM Psychiatrist Lrh-MhsGurvinder KalraNo ratings yet
- Text 1 (A & B)Document2 pagesText 1 (A & B)ifx leeNo ratings yet
- Bio 270 Lecture 10 University of TorontoDocument24 pagesBio 270 Lecture 10 University of TorontoJD BaruaNo ratings yet
- Maria 0001Document1 pageMaria 0001Irene Hail GingoyonNo ratings yet
- Organic InorganicDocument51 pagesOrganic InorganicPatrick GoNo ratings yet
- DOCEMY LEVEL I NOTES Compressed Lyst1719Document299 pagesDOCEMY LEVEL I NOTES Compressed Lyst1719nandaram2191No ratings yet
- Jurnal Katak PDFDocument5 pagesJurnal Katak PDF31122007No ratings yet
- FalciparumDocument4 pagesFalciparumDandun Dannie-DunNo ratings yet
- PERKECAMBAHAN BENIH PALA (Myristica Fragrans Houtt.) Dengan Metode Skarifikasi Dan Perendaman ZPT AlamiDocument11 pagesPERKECAMBAHAN BENIH PALA (Myristica Fragrans Houtt.) Dengan Metode Skarifikasi Dan Perendaman ZPT AlamiPutri HarahapNo ratings yet
- Saliva and Gastrointestinal FunctionsDocument13 pagesSaliva and Gastrointestinal FunctionsNizam Mischievous'Lovely Schremo BoyysNo ratings yet
- Zoology ReviewerDocument10 pagesZoology ReviewerJohn Gabrelle DoguilesNo ratings yet
- Increased Lactation Risk For Late Preterm InfantsDocument9 pagesIncreased Lactation Risk For Late Preterm InfantssmokaNo ratings yet
- Abdominal Compartment Syndrome A Case ReportDocument2 pagesAbdominal Compartment Syndrome A Case ReportEditor IJTSRDNo ratings yet
- Accessory Respiratory Organ-FishDocument63 pagesAccessory Respiratory Organ-Fishkaushik mallickNo ratings yet