You might also like
- Thermal Analysis V2: Inorganic Materials and Physical ChemistryFrom EverandThermal Analysis V2: Inorganic Materials and Physical ChemistryRobert F. Jr. SchwenkerRating: 1 out of 5 stars1/5 (1)
- ElecrolytesDocument4 pagesElecrolytesKrizzia Allyssa CotingjoNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Potassium DeterminationDocument1 pagePotassium DeterminationEl Marie SalungaNo ratings yet
- Electrolytes: Sodium (Na or Natrium)Document6 pagesElectrolytes: Sodium (Na or Natrium)Emmylou Murillo100% (1)
- Clinical Chemistry Lecture: Exercise, Training EffectsDocument3 pagesClinical Chemistry Lecture: Exercise, Training EffectsHenry QuimbaNo ratings yet
- Heat Coagulation TestDocument8 pagesHeat Coagulation TestRawan MaherNo ratings yet
- Basic Examination of BloodDocument6 pagesBasic Examination of BloodMadeleinePriscillaNo ratings yet
- Anti Anemia DrugsDocument36 pagesAnti Anemia DrugsArabelle GONo ratings yet
- BUN and CreatinineDocument4 pagesBUN and Creatininesarguss14100% (1)
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDocument25 pagesClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahNo ratings yet
- TRACE ELEMENTS: BIOLOGICAL FUNCTIONS AND IRON DEFICIENCY ANEMIADocument7 pagesTRACE ELEMENTS: BIOLOGICAL FUNCTIONS AND IRON DEFICIENCY ANEMIAVinNo ratings yet
- Classification of AnemiaDocument33 pagesClassification of Anemialieynna4996No ratings yet
- HaemoglobinDocument47 pagesHaemoglobinPreethi AbhilashNo ratings yet
- (CLINPATH) Lipids and DyslipoproteinemiaDocument5 pages(CLINPATH) Lipids and DyslipoproteinemiaJolaine ValloNo ratings yet
- Course Name:: Volumetric and Gravimetric Analytical Chemistry: 4022133-3Document37 pagesCourse Name:: Volumetric and Gravimetric Analytical Chemistry: 4022133-3faycalfaidiNo ratings yet
- A. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)Document19 pagesA. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)IceNo ratings yet
- AkiDocument13 pagesAkiharshe v100% (1)
- CC Lab 6 TransesDocument6 pagesCC Lab 6 TransesCiara PamonagNo ratings yet
- Structure of KidneysDocument36 pagesStructure of KidneysunisoldierNo ratings yet
- NPN ReviewDocument46 pagesNPN Reviewmika de guzmanNo ratings yet
- Thalassemi ADocument23 pagesThalassemi Ainterna MANADO100% (1)
- Kidney: Biochemical Tests For Assessing Renal FunctionsDocument56 pagesKidney: Biochemical Tests For Assessing Renal FunctionsPaulina Paskeviciute100% (1)
- Hyponatremia in Children 03.19.2010Document23 pagesHyponatremia in Children 03.19.2010Emily EresumaNo ratings yet
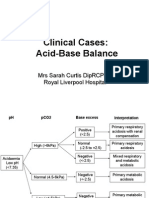
- Acid-Base BalanceDocument28 pagesAcid-Base Balanceps4only100% (1)
- Non Protein CompoundsDocument64 pagesNon Protein CompoundsAbigail Mayled LausNo ratings yet
- Shelly HyperlipidemiaDocument22 pagesShelly Hyperlipidemiaale marilNo ratings yet
- Pharmacology of Drugs For AnemiaDocument49 pagesPharmacology of Drugs For AnemiaTeus Fatamorgana100% (2)
- Case Histo PDFDocument19 pagesCase Histo PDFsomayya waliNo ratings yet
- Aub F Urine Screening For Metabolic DisordersDocument4 pagesAub F Urine Screening For Metabolic DisordersRomie SolacitoNo ratings yet
- Cardiac Function Tests: Example: Normal Formula LDH 1 2 0.5 LDH 2 4Document1 pageCardiac Function Tests: Example: Normal Formula LDH 1 2 0.5 LDH 2 4Ritz CelsoNo ratings yet
- CC Partii&III NotesDocument30 pagesCC Partii&III NotesAnielle Mongaya100% (1)
- UrinalysisDocument9 pagesUrinalysisSukma EffendyNo ratings yet
- Chem Lab 4 ElectrolytesDocument17 pagesChem Lab 4 ElectrolytesbiddyusmcNo ratings yet
- Activity 1 Reviewer - 2Document6 pagesActivity 1 Reviewer - 2Francis Zaccheau ValdezNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- Trace Elements in the BodyDocument21 pagesTrace Elements in the BodyJunea SeeNo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNo ratings yet
- 06.disorder of Carbohydrate MetabolismDocument47 pages06.disorder of Carbohydrate MetabolismRizka NizarNo ratings yet
- Diagrammatic Description of Blood Preparation ProcessesDocument17 pagesDiagrammatic Description of Blood Preparation ProcessesJes CmtNo ratings yet
- UV Absorbance: Click To Edit Master Subtitle StyleDocument24 pagesUV Absorbance: Click To Edit Master Subtitle StylePaula Denice Carlos BagunuNo ratings yet
- Sources of Errors in Clinical ChemistryDocument9 pagesSources of Errors in Clinical Chemistrykalantan23No ratings yet
- Why Is A Prothrombin Time Test Performed?: WarfarinDocument6 pagesWhy Is A Prothrombin Time Test Performed?: WarfarinMamta ShindeNo ratings yet
- SGOT ASAT Kit Reitman Frankel MethodDocument3 pagesSGOT ASAT Kit Reitman Frankel MethodShribagla MukhiNo ratings yet
- BiochemistryDocument135 pagesBiochemistryPradip HamalNo ratings yet
- Heme Metabolism PDFDocument19 pagesHeme Metabolism PDFAnonymous jW7BU44ACNo ratings yet
- Acid-Base MSC CasesDocument16 pagesAcid-Base MSC Casesmonday125No ratings yet
- Liver FunctionDocument30 pagesLiver FunctionAra ShirikaNo ratings yet
- Megaloblastic AnaemiaDocument11 pagesMegaloblastic AnaemiaJesmin_36No ratings yet
- Protein Metab 2 Dra. SantosDocument7 pagesProtein Metab 2 Dra. SantosMelissa SalayogNo ratings yet
- Kidney Nephron Structure and FunctionDocument4 pagesKidney Nephron Structure and Functionxanxan4321No ratings yet
- 2.biochemistry OSPEDocument55 pages2.biochemistry OSPEmermaidshruti1524No ratings yet
- Titration of Amino AcidsDocument21 pagesTitration of Amino AcidsCeleste Schepers0% (1)
- Lipid Profile: by Micheal and ChristianDocument15 pagesLipid Profile: by Micheal and ChristianMichealNo ratings yet
- Normocytic Anemia'sDocument14 pagesNormocytic Anemia'sbrown_chocolate87643No ratings yet
- Blood ComponentsDocument4 pagesBlood ComponentsRay Angelo RobidilloNo ratings yet
- Assessment of Acid-Base DisordersDocument39 pagesAssessment of Acid-Base Disordersmonday125100% (1)
- CC2 - Electrolytes and Inorganic IonsDocument4 pagesCC2 - Electrolytes and Inorganic Ionsjohnjoseph.ermitanoNo ratings yet
- Electrolyte 1Document8 pagesElectrolyte 1Ylooner QuitsNo ratings yet
- Research PrelimsDocument10 pagesResearch Prelimsjohnjoseph.ermitanoNo ratings yet
- CC2 - Tumor Markers and VitaminsDocument7 pagesCC2 - Tumor Markers and Vitaminsjohnjoseph.ermitanoNo ratings yet
- CC2 - Electrolytes and Inorganic IonsDocument4 pagesCC2 - Electrolytes and Inorganic Ionsjohnjoseph.ermitanoNo ratings yet
- Thyroid Thyroid GlandDocument3 pagesThyroid Thyroid Glandjohnjoseph.ermitanoNo ratings yet
- Carbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistryDocument93 pagesCarbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistrySimham Venu0% (1)
- Fluoric Acid - Allen HandbookDocument12 pagesFluoric Acid - Allen HandbookaldodiasNo ratings yet
- Maturity Onset Diabetes of The Young: Clinical Characteristics, Diagnosis and ManagementDocument10 pagesMaturity Onset Diabetes of The Young: Clinical Characteristics, Diagnosis and ManagementatikahanifahNo ratings yet
- Assessment and Management of Endo-Periodontal Lesions: DentistryDocument12 pagesAssessment and Management of Endo-Periodontal Lesions: Dentistryedgar curayNo ratings yet
- Scientific PapersDocument98 pagesScientific PapersZack MarksNo ratings yet
- Mind The Gap Final PDFDocument33 pagesMind The Gap Final PDFlmaoheartsNo ratings yet
- Pediatric Nursing Care PlanDocument18 pagesPediatric Nursing Care PlanRo Vin100% (2)
- The New York Times Magazine April 10 2016 PDFDocument62 pagesThe New York Times Magazine April 10 2016 PDFAaron ScottNo ratings yet
- Digoxin (Lanoxin)Document1 pageDigoxin (Lanoxin)ENo ratings yet
- Ancef Drug CardDocument1 pageAncef Drug CardSheri490No ratings yet
- All Uworld Notes 2019 Nclex Nursing ResourcesDocument152 pagesAll Uworld Notes 2019 Nclex Nursing Resourcesnene lewis100% (1)
- Case Presentation On Rheumatoid ArthritisDocument36 pagesCase Presentation On Rheumatoid ArthritisGADDAM TEJASWINI50% (2)
- Microbiology: Section IiDocument40 pagesMicrobiology: Section Iiparthibanb88100% (78)
- Drug Cheat SheetDocument6 pagesDrug Cheat SheetSheldon LordNo ratings yet
- Snakes RemediesDocument20 pagesSnakes RemediesAnkit SinhaNo ratings yet
- Diagnosis and Management of Electrolyte EmergenciesDocument29 pagesDiagnosis and Management of Electrolyte EmergenciesFatin Farhana JubaidiNo ratings yet
- DRUG-STUDY - CelecoxibDocument3 pagesDRUG-STUDY - Celecoxibamal abdulrahmanNo ratings yet
- CBD A Sick NeonateDocument36 pagesCBD A Sick NeonateAly MorsyNo ratings yet
- Dermatology Study Guide 2021Document5 pagesDermatology Study Guide 2021Osmo SisNo ratings yet
- Infective EndocarditisDocument3 pagesInfective EndocarditisRechelle CabagingNo ratings yet
- Colon CancerDocument2 pagesColon CancersweetyjonasNo ratings yet
- Journal of Oral and Maxillofacial Surgery - HealthFirstDocument333 pagesJournal of Oral and Maxillofacial Surgery - HealthFirstDodo AlvaNo ratings yet
- Breast History PDFDocument9 pagesBreast History PDFApurv GuptaNo ratings yet
- Phototherapy Induced Hypocalcemia in NeonatesDocument5 pagesPhototherapy Induced Hypocalcemia in Neonatesrandomized1234No ratings yet
- The Puerperium: Anatomic and Physiological Changes After BirthDocument66 pagesThe Puerperium: Anatomic and Physiological Changes After BirthCHALIE MEQUNo ratings yet
- Cogentin - Artane - Parlodel - Akineton - Benadryl - LarodopaDocument11 pagesCogentin - Artane - Parlodel - Akineton - Benadryl - LarodopaJoseph DavidNo ratings yet
- Cynara Scolymus ArtichokeDocument8 pagesCynara Scolymus Artichokeplanet_renNo ratings yet
- Psychiatric Nursing NotesDocument19 pagesPsychiatric Nursing NotesMarcus, RN100% (1)
- Atelectasis: CausesDocument4 pagesAtelectasis: Causesaznknight323No ratings yet
- Chronic Kidney Disease Stages, Risk Factors, and TreatmentDocument45 pagesChronic Kidney Disease Stages, Risk Factors, and Treatmentnaro ayosNo ratings yet
- Sully: The Untold Story Behind the Miracle on the HudsonFrom EverandSully: The Untold Story Behind the Miracle on the HudsonRating: 4 out of 5 stars4/5 (103)
- The Fabric of Civilization: How Textiles Made the WorldFrom EverandThe Fabric of Civilization: How Textiles Made the WorldRating: 4.5 out of 5 stars4.5/5 (57)
- Packing for Mars: The Curious Science of Life in the VoidFrom EverandPacking for Mars: The Curious Science of Life in the VoidRating: 4 out of 5 stars4/5 (1395)
- The Beekeeper's Lament: How One Man and Half a Billion Honey Bees Help Feed AmericaFrom EverandThe Beekeeper's Lament: How One Man and Half a Billion Honey Bees Help Feed AmericaNo ratings yet
- The Weather Machine: A Journey Inside the ForecastFrom EverandThe Weather Machine: A Journey Inside the ForecastRating: 3.5 out of 5 stars3.5/5 (31)
- Hero Found: The Greatest POW Escape of the Vietnam WarFrom EverandHero Found: The Greatest POW Escape of the Vietnam WarRating: 4 out of 5 stars4/5 (19)
- Faster: How a Jewish Driver, an American Heiress, and a Legendary Car Beat Hitler's BestFrom EverandFaster: How a Jewish Driver, an American Heiress, and a Legendary Car Beat Hitler's BestRating: 4 out of 5 stars4/5 (28)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (80)
- 35 Miles From Shore: The Ditching and Rescue of ALM Flight 980From Everand35 Miles From Shore: The Ditching and Rescue of ALM Flight 980Rating: 4 out of 5 stars4/5 (21)
- A Place of My Own: The Architecture of DaydreamsFrom EverandA Place of My Own: The Architecture of DaydreamsRating: 4 out of 5 stars4/5 (241)
- The Future of Geography: How the Competition in Space Will Change Our WorldFrom EverandThe Future of Geography: How the Competition in Space Will Change Our WorldRating: 4.5 out of 5 stars4.5/5 (4)
- Dirt to Soil: One Family’s Journey into Regenerative AgricultureFrom EverandDirt to Soil: One Family’s Journey into Regenerative AgricultureRating: 5 out of 5 stars5/5 (124)
- Pale Blue Dot: A Vision of the Human Future in SpaceFrom EverandPale Blue Dot: A Vision of the Human Future in SpaceRating: 4.5 out of 5 stars4.5/5 (586)
- Across the Airless Wilds: The Lunar Rover and the Triumph of the Final Moon LandingsFrom EverandAcross the Airless Wilds: The Lunar Rover and the Triumph of the Final Moon LandingsNo ratings yet
- Data-ism: The Revolution Transforming Decision Making, Consumer Behavior, and Almost Everything ElseFrom EverandData-ism: The Revolution Transforming Decision Making, Consumer Behavior, and Almost Everything ElseRating: 3.5 out of 5 stars3.5/5 (12)
- Recording Unhinged: Creative and Unconventional Music Recording TechniquesFrom EverandRecording Unhinged: Creative and Unconventional Music Recording TechniquesNo ratings yet
- Einstein's Fridge: How the Difference Between Hot and Cold Explains the UniverseFrom EverandEinstein's Fridge: How the Difference Between Hot and Cold Explains the UniverseRating: 4.5 out of 5 stars4.5/5 (50)
- Reality+: Virtual Worlds and the Problems of PhilosophyFrom EverandReality+: Virtual Worlds and the Problems of PhilosophyRating: 4 out of 5 stars4/5 (24)
- The Technology Trap: Capital, Labor, and Power in the Age of AutomationFrom EverandThe Technology Trap: Capital, Labor, and Power in the Age of AutomationRating: 4.5 out of 5 stars4.5/5 (46)
- Broken Money: Why Our Financial System is Failing Us and How We Can Make it BetterFrom EverandBroken Money: Why Our Financial System is Failing Us and How We Can Make it BetterRating: 5 out of 5 stars5/5 (3)
- Fallout: The Hiroshima Cover-up and the Reporter Who Revealed It to the WorldFrom EverandFallout: The Hiroshima Cover-up and the Reporter Who Revealed It to the WorldRating: 4.5 out of 5 stars4.5/5 (82)
- The Path Between the Seas: The Creation of the Panama Canal, 1870-1914From EverandThe Path Between the Seas: The Creation of the Panama Canal, 1870-1914Rating: 4.5 out of 5 stars4.5/5 (124)