You might also like
- Zero To Finals MedicineDocument352 pagesZero To Finals MedicinePlay100% (23)
- PracticeExam CCSDocument12 pagesPracticeExam CCSBehrouz Yari75% (4)
- LPN DELEGATION and PRIORITIZING AND MOREDocument38 pagesLPN DELEGATION and PRIORITIZING AND MOREDebra PowellNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For HypertensionJessy MalloNo ratings yet
- Protocol 13: Chest Pain: A&E DoctorDocument4 pagesProtocol 13: Chest Pain: A&E DoctorVanessa HermioneNo ratings yet
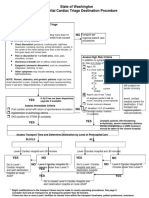
- State of Washington Prehospital Cardiac Triage Destination ProcedureDocument4 pagesState of Washington Prehospital Cardiac Triage Destination ProcedureNanda Dwi Bintoro ZiehenShopNo ratings yet
- Week 5 ChestPain Student HODocument8 pagesWeek 5 ChestPain Student HOVindicated ReignNo ratings yet
- Cardio BBDocument73 pagesCardio BBايات عبدالرحمنNo ratings yet
- Chest Pain Protocol in EDDocument3 pagesChest Pain Protocol in EDshahidchaudharyNo ratings yet
- KillipsDocument12 pagesKillipsNhorlyn Adante SoltesNo ratings yet
- ACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyDocument30 pagesACLS Secondary Survey For A Patient in Respiratory Arrest: BLS Arrest Figure 1. Basic Life Support Primary SurveyLusia NataliaNo ratings yet
- ACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesDocument2 pagesACLS-Pediatric Wide Complex Tachycardia: Sample Medical GuidelinesFebrialitaFatoniNo ratings yet
- Unstable AnginaDocument5 pagesUnstable AnginaAria AlysisNo ratings yet
- Maternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Document2 pagesMaternal Tachycardia Management Pathway at Health Clinic in Pahang 2022Yash atriNo ratings yet
- Advanced Cardiac Life Support (Acls) Part Iii: ACP 202 Module 6Document39 pagesAdvanced Cardiac Life Support (Acls) Part Iii: ACP 202 Module 6MoeNo ratings yet
- Assessment of The Acutely Ill PatientDocument10 pagesAssessment of The Acutely Ill PatientZacmilo Dela TorreNo ratings yet
- Preop Eval '14 UpdateDocument33 pagesPreop Eval '14 UpdateRed DevilNo ratings yet
- PrioritizationDocument20 pagesPrioritizationPascal St Peter Nwaorgu100% (1)
- NP Case Example TwoDocument5 pagesNP Case Example TwoAnisaNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- Diana Pefbrianti, S.Kep., NS., M.KepDocument33 pagesDiana Pefbrianti, S.Kep., NS., M.KepMursidah faNo ratings yet
- Tony Cross CDU Low Risk ACS Proforma - V3.212 Review Due June 2014Document4 pagesTony Cross CDU Low Risk ACS Proforma - V3.212 Review Due June 2014ED@HEFTNo ratings yet
- Cardiac Case StudyDocument12 pagesCardiac Case StudyEdwin Delos Reyes Abu100% (1)
- Acute Coronary Syndromes AlgorithmDocument5 pagesAcute Coronary Syndromes AlgorithmLiuk IrawatiNo ratings yet
- Acute Myocardial Infarction: QuestionsDocument18 pagesAcute Myocardial Infarction: QuestionsAbdul QuyyumNo ratings yet
- Chest Pain: Sumit Bose, MD PGY-3Document55 pagesChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- Anesthesia Pre Operative EvaluationDocument27 pagesAnesthesia Pre Operative EvaluationHassan.shehri100% (2)
- Coronary Artery Disease: Aleson Claire A. Llanes, MDDocument94 pagesCoronary Artery Disease: Aleson Claire A. Llanes, MDFly LlanesNo ratings yet
- Arterial Septal Defect (Asd)Document38 pagesArterial Septal Defect (Asd)Rhahima SyafrilNo ratings yet
- Acute Coronary Syndrome (ACS) : Basic Principles For ACSDocument4 pagesAcute Coronary Syndrome (ACS) : Basic Principles For ACSRendra DananjayaNo ratings yet
- PGY1 Survival SkillsDocument22 pagesPGY1 Survival SkillsΓρε ΓορυNo ratings yet
- "Bad Heartburn" 82 Yo Female Without Chest Pain: Uncategorized Brooks Walsh MD 9 CommentsDocument1 page"Bad Heartburn" 82 Yo Female Without Chest Pain: Uncategorized Brooks Walsh MD 9 CommentsRichard SiahaanNo ratings yet
- ST-Elevation: N N N N N N N NDocument5 pagesST-Elevation: N N N N N N N NningputNo ratings yet
- ST Segment Elevated Myocardiac Infarction (Stemi) ObjectivesDocument25 pagesST Segment Elevated Myocardiac Infarction (Stemi) ObjectivesWilliam Yap WLNo ratings yet
- Nyeri DadaDocument27 pagesNyeri DadaAji Setia UtamaNo ratings yet
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDocument34 pagesUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- Ischemic Heart DiseaseDocument8 pagesIschemic Heart Diseaseiri_balNo ratings yet
- Preoperative AssessmentDocument2 pagesPreoperative AssessmentTom MallinsonNo ratings yet
- Triage in The Emergency Department 1Document17 pagesTriage in The Emergency Department 1Christine Joy MuñozNo ratings yet
- Cardio Vascular Disease in PregnancyDocument57 pagesCardio Vascular Disease in PregnancySanthosh.S.U0% (1)
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- Management of Common Cases in Emergency MedicineDocument55 pagesManagement of Common Cases in Emergency MedicinemonpyitharNo ratings yet
- Clinical Guideline For Management of Acute Pancreatitis in AdultsDocument13 pagesClinical Guideline For Management of Acute Pancreatitis in AdultsrivaldiNo ratings yet
- Approach To Chest PainDocument52 pagesApproach To Chest PainChris Jardine LiNo ratings yet
- Chest Pain On The WardsDocument58 pagesChest Pain On The WardsNikNo ratings yet
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- Acls UpdatedDocument37 pagesAcls UpdatedrigasanaorayNo ratings yet
- Chest Pain Pres WebinarDocument28 pagesChest Pain Pres Webinarteukureza fatwaNo ratings yet
- 9 - The Cardiovascular AssessmentDocument54 pages9 - The Cardiovascular Assessmente.mb275No ratings yet
- Valvular Heart Disease:: Ambulatory Monitoring and Surgical ReferralDocument56 pagesValvular Heart Disease:: Ambulatory Monitoring and Surgical ReferralAndi Suchy Qumala SarieNo ratings yet
- Advanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6Document32 pagesAdvanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6MoeNo ratings yet
- Activtiy UntitledDocument6 pagesActivtiy UntitledJan Cyrel ColomaNo ratings yet
- Acute Coronary SyndromeDocument41 pagesAcute Coronary SyndromeAbdulhameed MohamedNo ratings yet
- Evidence-Based Practice of Anesthesiology Chapter 2: Update On Preprocedure TestingDocument2 pagesEvidence-Based Practice of Anesthesiology Chapter 2: Update On Preprocedure Testingrtaneja92No ratings yet
- CCS - Handbook of Anesthesiology (2005)Document180 pagesCCS - Handbook of Anesthesiology (2005)Rojelle LezamaNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- Sacubitril Valsartan The Role of NeprilyDocument11 pagesSacubitril Valsartan The Role of NeprilySalvanabilaNo ratings yet
- Thesis On Coronary Heart DiseaseDocument7 pagesThesis On Coronary Heart Diseasetracyclarkwarren100% (1)
- 2006 Feb Inpatient Quality IndicatorsDocument1 page2006 Feb Inpatient Quality IndicatorsJPNo ratings yet
- Blood Pressure Control InType 2 DiabetesDocument119 pagesBlood Pressure Control InType 2 Diabetesjourey08No ratings yet
- Cerebral AneurysmDocument24 pagesCerebral Aneurysmcaptain_rafeNo ratings yet
- Simpo 14 Sept 19Document71 pagesSimpo 14 Sept 19Henry SNo ratings yet
- Basis of ECG and Intro To ECG InterpretationDocument10 pagesBasis of ECG and Intro To ECG InterpretationKristin SmithNo ratings yet
- PeripheralVascularDisease NotesDocument6 pagesPeripheralVascularDisease NotesNoah PontinoNo ratings yet
- Discharge PlanDocument2 pagesDischarge PlanHannah ChiuNo ratings yet
- Activity 7 The Cardiovascular SystemDocument4 pagesActivity 7 The Cardiovascular SystemEllen Mynelle MabulacNo ratings yet
- Form 3 Science Chapter 2Document9 pagesForm 3 Science Chapter 2Mohamad Harith100% (5)
- Transport of Substances in Humans (LQ)Document13 pagesTransport of Substances in Humans (LQ)Wan Ching ChanNo ratings yet
- Wesley Purkey AutopsyDocument2 pagesWesley Purkey AutopsyEthan BiandoNo ratings yet
- Review Sheet AP2 Test #1 (19, 20 & 21) EXAM 1Document2 pagesReview Sheet AP2 Test #1 (19, 20 & 21) EXAM 1Charity KiplagatNo ratings yet
- Form 3 Science Chap3-TransportationDocument33 pagesForm 3 Science Chap3-TransportationYeLynTan100% (1)
- Global Surgical PeriodsDocument4 pagesGlobal Surgical PeriodsRashiden MadjalesNo ratings yet
- European Heart Journal Supplements (2019) - SeptemberDocument82 pagesEuropean Heart Journal Supplements (2019) - SeptemberBeard BeardNo ratings yet
- (Junjie Xiao (Eds.) ) Exercise For Cardiovascular D (B-Ok - CC)Document380 pages(Junjie Xiao (Eds.) ) Exercise For Cardiovascular D (B-Ok - CC)Nacido para BendcirNo ratings yet
- Syok Kardiogenik Dr. Rani Maliawan, SP JPDocument59 pagesSyok Kardiogenik Dr. Rani Maliawan, SP JPLuh Leni AriniNo ratings yet
- CH 19 Transport in HumanDocument49 pagesCH 19 Transport in HumanRay PeramathevanNo ratings yet
- Diara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineDocument19 pagesDiara Jossiean M. Rogacion: Clinical Clerk 2020-2021 Group 5B Department of MedicineJara RogacionNo ratings yet
- Unstable AnginaDocument11 pagesUnstable AnginaAdrian BoboceaNo ratings yet
- RLE NCMB 314-M2-CU8 Cardiovascular ChangesDocument5 pagesRLE NCMB 314-M2-CU8 Cardiovascular ChangesJordz PlaciNo ratings yet
- Coronary Artery Bypass GraftingDocument9 pagesCoronary Artery Bypass GraftingRickCohen100% (1)
- Web Path AllDocument116 pagesWeb Path AllFYM0% (1)
- Soal MCQ Dari EJVESDocument4 pagesSoal MCQ Dari EJVESAnonymous 7I3ns1zTCNo ratings yet
- Lesson 3 Hemodynamic Monitoring Semi Finals 3Document18 pagesLesson 3 Hemodynamic Monitoring Semi Finals 3Juffer ConconNo ratings yet
- Causes of Brain DamageDocument2 pagesCauses of Brain Damagejanlyn espinosaNo ratings yet