You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Melanin What Makes Black People Black by Llaila Afrika PDF TextDocument37 pagesMelanin What Makes Black People Black by Llaila Afrika PDF Textkiki crystal (ImmaAMENTIgoddess)No ratings yet
- SCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Document46 pagesSCIENCE-10-Q3 WORKSHEET REVISED COPY-week-1-7Gian Evangelista67% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Unit 3 Study GuideDocument10 pagesUnit 3 Study GuideangieswensonNo ratings yet
- The AMC Notes Practice Test (150 Sample Questions)Document113 pagesThe AMC Notes Practice Test (150 Sample Questions)Gofi100% (1)
- Midterm Exams - AnatomyDocument9 pagesMidterm Exams - AnatomyBing58No ratings yet
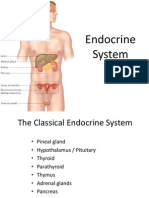
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (3)
- OkxygenDocument5 pagesOkxygenJokevin PrasetyadhiNo ratings yet
- The Most Important Throat-Related Symptoms Suggestive of Chronic Tonsillitis As The Main Indication For Adult TonsillectomyDocument4 pagesThe Most Important Throat-Related Symptoms Suggestive of Chronic Tonsillitis As The Main Indication For Adult TonsillectomyJokevin PrasetyadhiNo ratings yet
- Pa Sample QuestionsDocument1 pagePa Sample QuestionsJokevin Prasetyadhi100% (1)
- ICD 10 Most Common UrologyDocument4 pagesICD 10 Most Common UrologyJokevin PrasetyadhiNo ratings yet
- Inversio UteriDocument4 pagesInversio UteriJokevin PrasetyadhiNo ratings yet
- Motor PhenotypesDocument42 pagesMotor PhenotypesJokevin PrasetyadhiNo ratings yet
- GoutDocument6 pagesGoutJokevin PrasetyadhiNo ratings yet
- MODULE 2.1 Antepartum - Pregnancy NURSING NOTESDocument11 pagesMODULE 2.1 Antepartum - Pregnancy NURSING NOTESQwer TyNo ratings yet
- Somaia Noman Rema Alqadhi Labiba Mohammed Lamia AlkamaliDocument26 pagesSomaia Noman Rema Alqadhi Labiba Mohammed Lamia AlkamaliAhmed AL-shaabiNo ratings yet
- Sample Paper 2Document17 pagesSample Paper 2Soham's Smart ShowNo ratings yet
- Complete Steroid Handbook 2004 EditionDocument82 pagesComplete Steroid Handbook 2004 Editionmathiouem100% (13)
- Human Physiology The Basic of MedicineDocument1,816 pagesHuman Physiology The Basic of Medicinebranislava_vuković100% (3)
- Biology ExamDocument2 pagesBiology ExamZephieNo ratings yet
- Physiology of The Endocrine and Nervous Systems 2017Document169 pagesPhysiology of The Endocrine and Nervous Systems 2017Criss CristinaNo ratings yet
- Cambridge O Level: Biology 5090/12Document20 pagesCambridge O Level: Biology 5090/12skrrt SkrrrttNo ratings yet
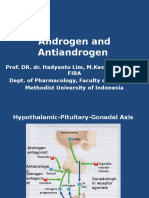
- Androgen and AntiandrogenDocument18 pagesAndrogen and AntiandrogenIrma MarianyNo ratings yet
- Intersex & Ambigous Genitalia Pediatric UrologyDocument26 pagesIntersex & Ambigous Genitalia Pediatric Urologyhayssam rashwanNo ratings yet
- European Association of Urology Guidelines 2021Document25 pagesEuropean Association of Urology Guidelines 2021Rares SanduNo ratings yet
- Pituitary and ThyroidDocument54 pagesPituitary and ThyroidSaif AliNo ratings yet
- Conversion Kit Price List: Ford Fiesta R2T v.2Document23 pagesConversion Kit Price List: Ford Fiesta R2T v.2crisate2544587100% (1)
- Heterophilic Antibody Interference Affecting Multiple Hormone Assays: Is It Due To Rheumatoid Factor?Document4 pagesHeterophilic Antibody Interference Affecting Multiple Hormone Assays: Is It Due To Rheumatoid Factor?mayra almaNo ratings yet
- FinalDocument3 pagesFinalAnupam Saraf IINo ratings yet
- Have You Reached The Age of "Adolescence"?Document14 pagesHave You Reached The Age of "Adolescence"?venkataNo ratings yet
- PregnylDocument4 pagesPregnylAdina DraghiciNo ratings yet
- Pregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDocument74 pagesPregnancy Handbook: "Am I Pregnant?" All B-HCG Levels ExplainedDr0Web100% (1)
- Irfan Mir Physiology Usmle Step 1Document37 pagesIrfan Mir Physiology Usmle Step 1sammieahemdNo ratings yet
- Ag Lstock Lecture Notes On Chicken Farming in Warm Climate Zones en 111220Document128 pagesAg Lstock Lecture Notes On Chicken Farming in Warm Climate Zones en 111220John Diete-Koki100% (1)
- Endocrine SystemDocument5 pagesEndocrine SystemKimberly Anne SP Padilla100% (2)
- Infertility in Farm AnimalsDocument20 pagesInfertility in Farm AnimalsИгор ГалоскиNo ratings yet
- 123 Human Reproduction NCERTDocument20 pages123 Human Reproduction NCERTtashukumar33No ratings yet
- Anexure IDocument3 pagesAnexure IJAGADISH PHARMACEUTICALS0% (1)