0% found this document useful (0 votes)
433 views6 pagesAAC for Individuals with Disabilities
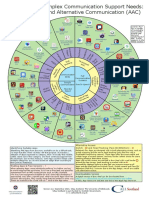
Augmentative-alternative communication (AAC) provides individuals with special needs a means of communication. The goals of AAC are to increase independence through expressing needs and enhancing communication skills. AAC devices must provide accessibility tailored to individual needs. AAC can take many forms, from manual communication to low and high-tech systems. It aims to make communication possible for those who have difficulty speaking, including those who are deaf/hard of hearing, have neurological impairments, progressive neurological disorders, autism, motor speech disorders, or neurogenetic disorders. AAC ranges from unaided forms like gestures to aided forms incorporating pictures, writing, communication boards, and electronic devices.
Uploaded by
Denisse Paz Hurtado BravoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
433 views6 pagesAAC for Individuals with Disabilities
Augmentative-alternative communication (AAC) provides individuals with special needs a means of communication. The goals of AAC are to increase independence through expressing needs and enhancing communication skills. AAC devices must provide accessibility tailored to individual needs. AAC can take many forms, from manual communication to low and high-tech systems. It aims to make communication possible for those who have difficulty speaking, including those who are deaf/hard of hearing, have neurological impairments, progressive neurological disorders, autism, motor speech disorders, or neurogenetic disorders. AAC ranges from unaided forms like gestures to aided forms incorporating pictures, writing, communication boards, and electronic devices.
Uploaded by
Denisse Paz Hurtado BravoCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Augmentative–Alternative Communication
- Forms of AAC
- Assessing the Need for AAC
- Assessing Communication Partners
- Using the AAC Device in Classroom or Home and Community Settings