You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Dean Spade, Mutilating GenderDocument23 pagesDean Spade, Mutilating GenderRebecca KuklaNo ratings yet
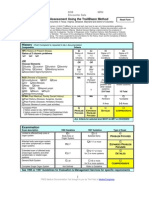
- Trailblazer Medicare Audit ToolDocument4 pagesTrailblazer Medicare Audit Tooladultmedicalconsultants100% (10)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NCP CholelithiasisDocument6 pagesNCP CholelithiasisAllan Macacapagal0% (1)
- Post Traumatic Stress DisorderDocument2 pagesPost Traumatic Stress Disorderapi-188978784100% (1)
- A Strange Case of Agoraphobia A Case StudyDocument4 pagesA Strange Case of Agoraphobia A Case StudyChhanak Agarwal100% (1)
- Shanghai Score System For Diagnosis of Brugada Syndrome PDFDocument7 pagesShanghai Score System For Diagnosis of Brugada Syndrome PDFFendy WellenNo ratings yet
- Legal and Ethical Issues in Medical PracticeDocument22 pagesLegal and Ethical Issues in Medical PracticeSagar Tanna100% (4)
- NPDDocument2 pagesNPDkuro hanabusaNo ratings yet
- Diagnosi S: MalariaDocument28 pagesDiagnosi S: MalariaOm Prakash SinghNo ratings yet
- DR Robert Stern Declaration in Support of Objection To NFL Concussion Settlement OfferDocument61 pagesDR Robert Stern Declaration in Support of Objection To NFL Concussion Settlement OfferRobert LeeNo ratings yet
- AbstractsDocument7 pagesAbstractsPuji YuliastriNo ratings yet
- Diagnostic Standards and Classification of Tuberculosis: CDC WonderDocument20 pagesDiagnostic Standards and Classification of Tuberculosis: CDC Wondereloi moliNo ratings yet
- PhobiasDocument12 pagesPhobiasAncaNo ratings yet
- Mapeh ReviewerDocument9 pagesMapeh ReviewerJulianne FNo ratings yet
- BSW Field Manual PDFDocument53 pagesBSW Field Manual PDFAnanta ChaliseNo ratings yet
- Antibiotic Induced Black Hairy TongueDocument11 pagesAntibiotic Induced Black Hairy TongueYuganya SriNo ratings yet
- Advances in Psychiatry Second VolumeDocument301 pagesAdvances in Psychiatry Second VolumeAlice Douglas100% (3)
- Presented byDocument57 pagesPresented byMB AamerNo ratings yet
- NRSG 100 Introduction To NursingDocument104 pagesNRSG 100 Introduction To Nursingchet_sisal7573No ratings yet
- Article by Shahrukh KhanDocument8 pagesArticle by Shahrukh Khanshahrukh khanNo ratings yet
- Handbook ADHD StudențiDocument134 pagesHandbook ADHD Studențimihaela neacsu100% (2)
- Beck Anxiety Inventory: From Wikipedia, The Free EncyclopediaDocument5 pagesBeck Anxiety Inventory: From Wikipedia, The Free EncyclopediaSrishti GaurNo ratings yet
- Oxford S Teaching Methods of English Language The Use of GamesDocument37 pagesOxford S Teaching Methods of English Language The Use of GamesGabdullina MairaNo ratings yet
- PSYCH-1.1C Quick Review Table-Schizo - Other Psychotic DisorderDocument1 pagePSYCH-1.1C Quick Review Table-Schizo - Other Psychotic DisorderMaikka IlaganNo ratings yet
- Establish of Vetigo. The Practitioner September 2010 - 254 (1732) : 19-23. 2010Document2 pagesEstablish of Vetigo. The Practitioner September 2010 - 254 (1732) : 19-23. 2010Langlang BawonoNo ratings yet
- Clinical Practice Guideline BPPVDocument47 pagesClinical Practice Guideline BPPVAnggaRusdiantoNo ratings yet
- Example of Expert SystemDocument5 pagesExample of Expert SystemJeremie BongatNo ratings yet
- Essentials of Preclinical Cons DentistryDocument333 pagesEssentials of Preclinical Cons DentistryChirayuNo ratings yet
- Activity 4Document7 pagesActivity 4Mary Rose Silva GargarNo ratings yet
- Psychological DisordersDocument48 pagesPsychological Disordersapi-448144386100% (1)